

A long diagnostic delay in patients with Hereditary Haemorrhagic Telangiectasia: a questionnaire-based retrospective study
- PMID: 22676497
- PMCID: PMC3458963
- DOI: 10.1186/1750-1172-7-33
A long diagnostic delay in patients with Hereditary Haemorrhagic Telangiectasia: a questionnaire-based retrospective study
Abstract
Background: The difficulty in establishing a timely correct diagnosis is a relevant matter of concern for several rare diseases. Many rare-disease-affected patients suffer from considerable diagnostic delay, mainly due to their poor knowledge among healthcare professionals, insufficient disease awareness among patients' families, and lack of promptly available diagnostic tools. Hereditary Haemorrhagic Telangiectasia (HHT) is an autosomal-dominantly inherited vascular dysplasia, affecting 1:5,000-10,000 patients. HHT is characterized by high variability of clinical manifestations, which show remarkable overlapping with several common diseases.
Aim: To perform a detailed analysis concerning the diagnostic time lag occurring in patients with HHT, defined as the time period spanning from the first clinical manifestation to the attainment of a definite, correct diagnosis.
Methods: A questionnaire was administered to the HHT patients previously recruited from 2000 and 2009. Clinical onset, first referral to a physician for disease manifestations, and first correct diagnosis of definite HHT were collected. Eventual misdiagnosis at first referral and serious complications occurring throughout the time elapsing between disease onset and definite diagnosis were also addressed.
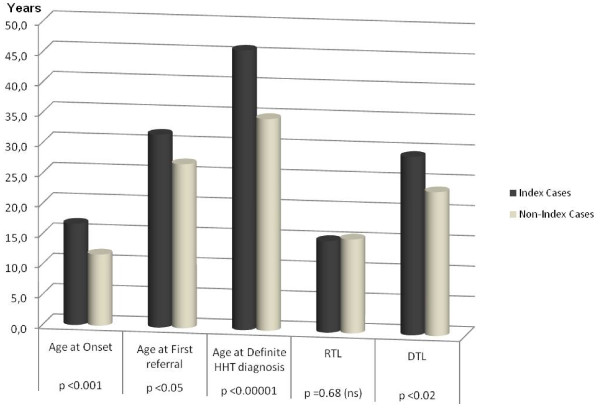
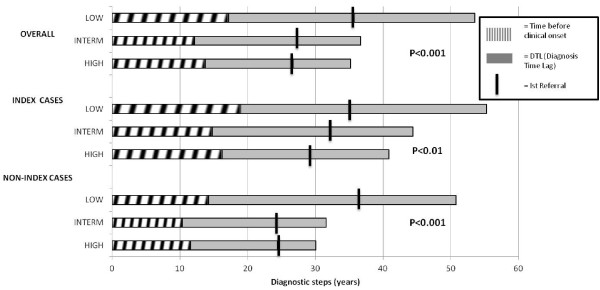
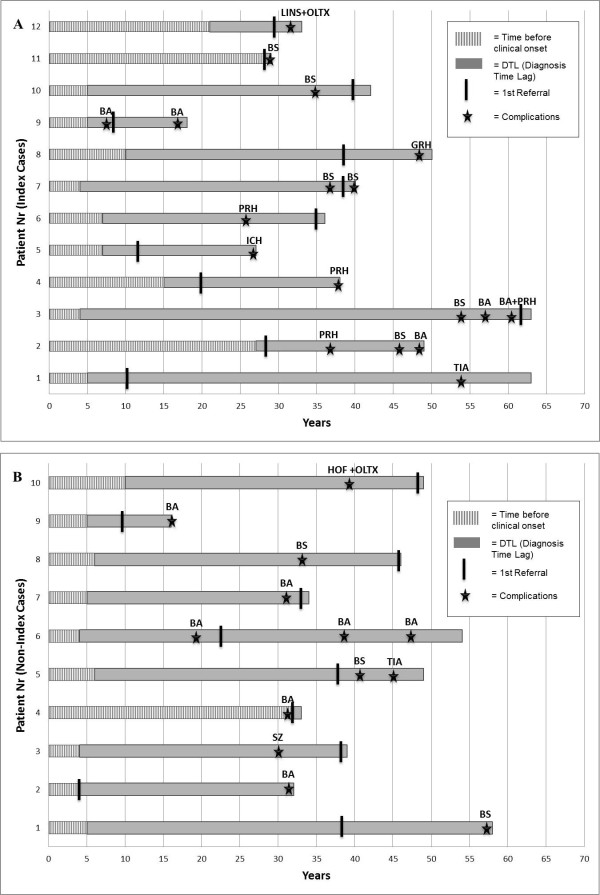
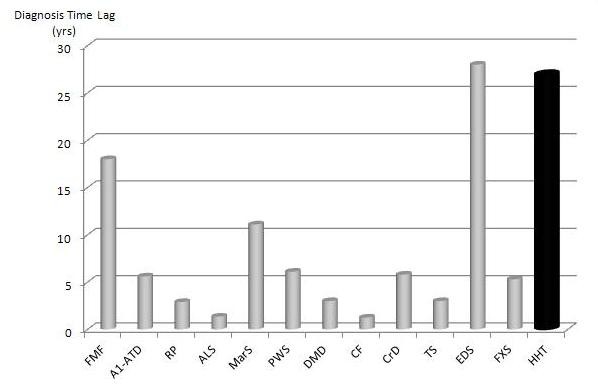
Results: In the 233 respondents, the clinical onset of disease occurred at an age of 14.1 yrs, while the age of first referral and the age of first definite diagnosis of HHT were 29.2 yrs and 40.1 yrs, respectively. Only 88/233 patients received a correct diagnosis at first counseling. Thus, the diagnostic time lag, represented by the time elapsing from disease onset and first definite diagnosis of HHT, proved to be 25.7 yrs. Twenty-two patients suffered from severe complications during this time interval. The diagnostic delay was significantly longer (p < 0.001) in index patients (first patients who attained definite HHT diagnosis in a given family) than in non-index patients (relative of index patients). The diagnostic time lag was also significantly associated with education grade (p < 0.001).
Conclusions: Our data report for the first time a systematic inquiry of diagnostic delay in HHT showing that patients receive a definite diagnosis only after nearly three decades from disease onset. Concerted efforts are still to be made to increase awareness of this disease among both families and physicians.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
