

Autonomic and hemodynamic origins of pre-hypertension: central role of heredity
- PMID: 22676942
- PMCID: PMC3374873
- DOI: 10.1016/j.jacc.2012.02.040
Autonomic and hemodynamic origins of pre-hypertension: central role of heredity
Abstract
Objectives: The purpose of this study is to better understand the origins and progression of pre-hypertension.
Background: Pre-hypertension is a risk factor for progression to hypertension, cardiovascular disease, and increased mortality. We used a cross-sectional twin study design to examine the role of heredity in likely pathophysiological events (autonomic or hemodynamic) in pre-hypertension.
Methods: Eight hundred twelve individuals (337 normotensive, 340 pre-hypertensive, 135 hypertensive) were evaluated in a sample of twin pairs, their siblings, and other family members. They underwent noninvasive hemodynamic, autonomic, and biochemical testing, as well as estimates of trait heritability (the percentage of trait variance accounted for by heredity) and pleiotropy (the genetic covariance or shared genetic determination of traits) by variance components.
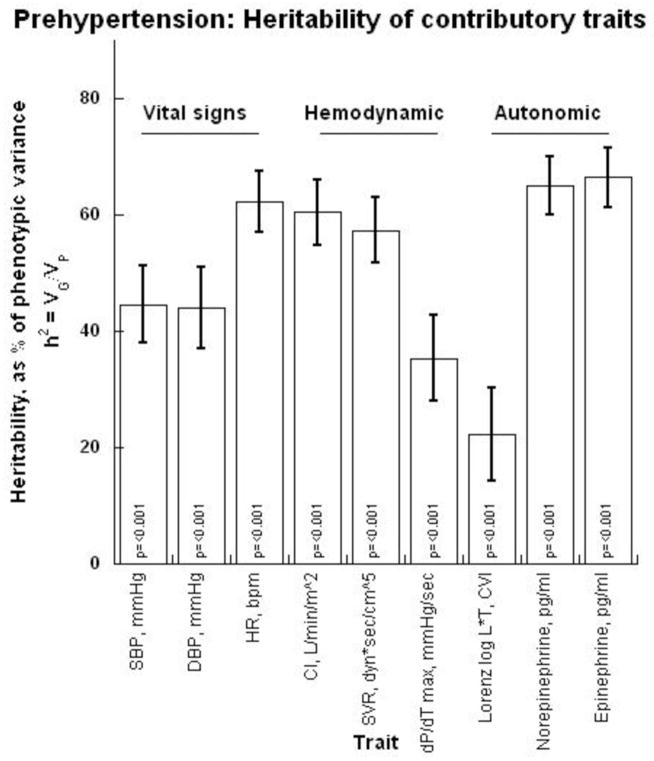
Results: In the hemodynamic realm, an elevation of cardiac contractility prompted increased stroke volume, in turn increasing cardiac output, which elevated blood pressure into the pre-hypertension range. Autonomic monitoring detected an elevation of norepinephrine secretion plus a decline in cardiac parasympathetic tone. Twin pair variance components documented substantial heritability as well as joint genetic determination for blood pressure and the contributory autonomic and hemodynamic traits. Genetic variation at a pathway locus also indicated pleiotropic effects on contractility and blood pressure.
Conclusions: Elevated blood pressure in pre-hypertension results from increased cardiac output, driven by contractility as well as heart rate, which may reflect both diminished parasympathetic and increased sympathetic tone. In the face of increased cardiac output, systemic vascular resistance fails to decline homeostatically. Such traits display substantial heritability and shared genetic determination, although by loci not yet elucidated. These findings clarify the role of heredity in the origin of pre-hypertension and its autonomic and hemodynamic pathogenesis. The results also establish pathways that suggest new therapeutic targets for pre-hypertension, or approaches to its prevention.
Copyright © 2012 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures









Comment in
-
Pre-hypertension and hyperkinetic heart (Gorlin's) syndrome: is there a parallel?J Am Coll Cardiol. 2012 Dec 4;60(22):2342. doi: 10.1016/j.jacc.2012.07.061. J Am Coll Cardiol. 2012. PMID: 23194950 No abstract available.
References
-
- Chobanian AV, Bakris GL, Black HR, et al. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report. Jama. 2003;289:2560–72. - PubMed
-
- Qureshi AI, Suri MF, Kirmani JF, Divani AA. Prevalence and trends of prehypertension and hypertension in United States: National Health and Nutrition Examination Surveys 1976 to 2000. Med Sci Monit. 2005;11:CR403–9. - PubMed
-
- Vasan RS, Larson MG, Leip EP, Kannel WB, Levy D. Assessment of frequency of progression to hypertension in non-hypertensive participants in the Framingham Heart Study: a cohort study. Lancet. 2001;358:1682–6. - PubMed
-
- Ogunniyi MO, Croft JB, Greenlund KJ, Giles WH, Mensah GA. Racial/ethnic differences in microalbuminuria among adults with prehypertension and hypertension: National Health and Nutrition Examination Survey (NHANES), 1999–2006. Am J Hypertens. 2010;23:859–64. - PubMed
-
- Ishikawa Y, Ishikawa J, Ishikawa S, et al. Prehypertension and the risk for cardiovascular disease in the Japanese general population: the Jichi Medical School Cohort Study. J Hypertens. 2010;28:1630–7. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
