

Pathology after eculizumab in dense deposit disease and C3 GN
- PMID: 22677550
- PMCID: PMC3380652
- DOI: 10.1681/ASN.2011121186
Pathology after eculizumab in dense deposit disease and C3 GN
Abstract
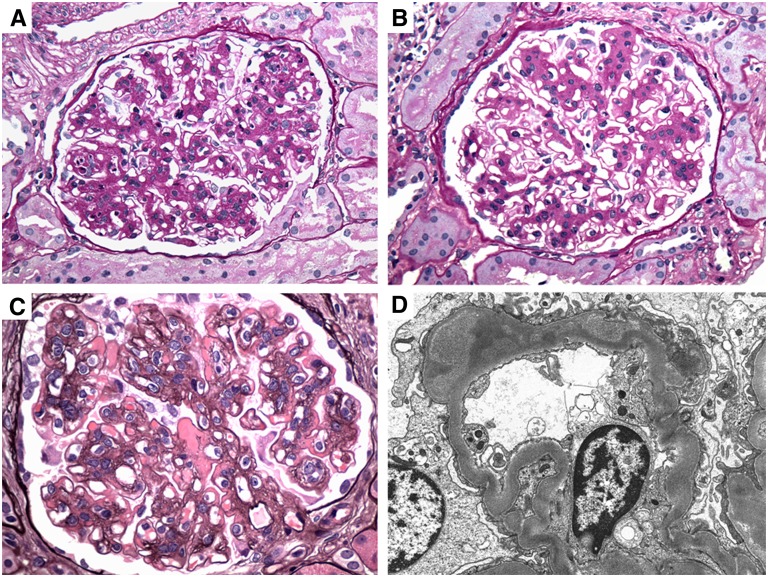
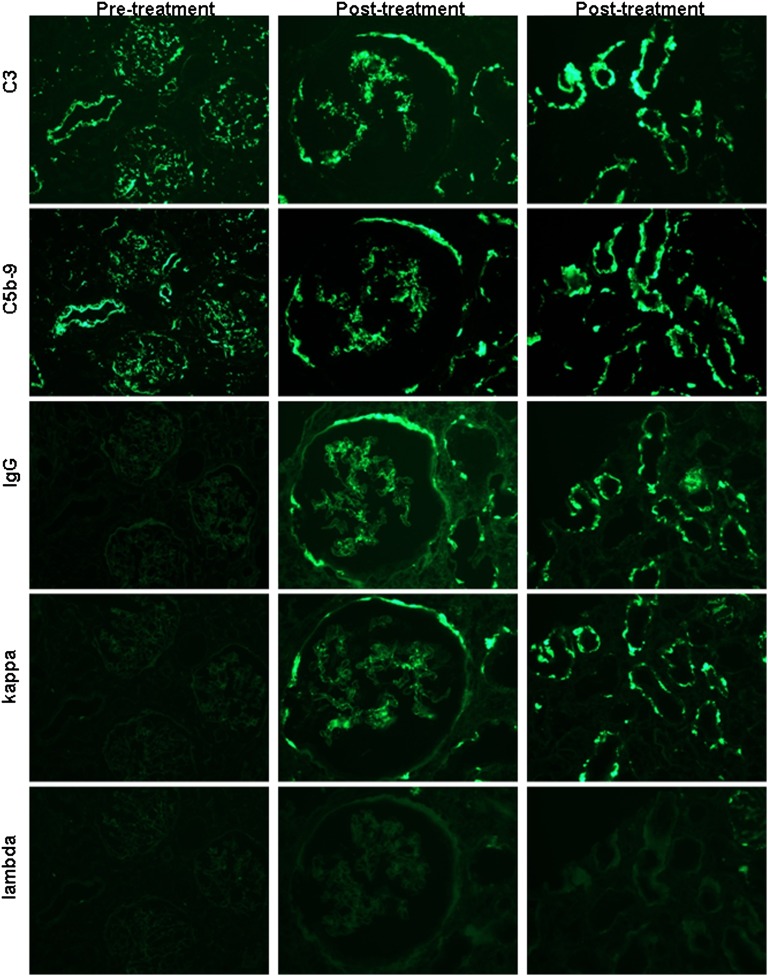
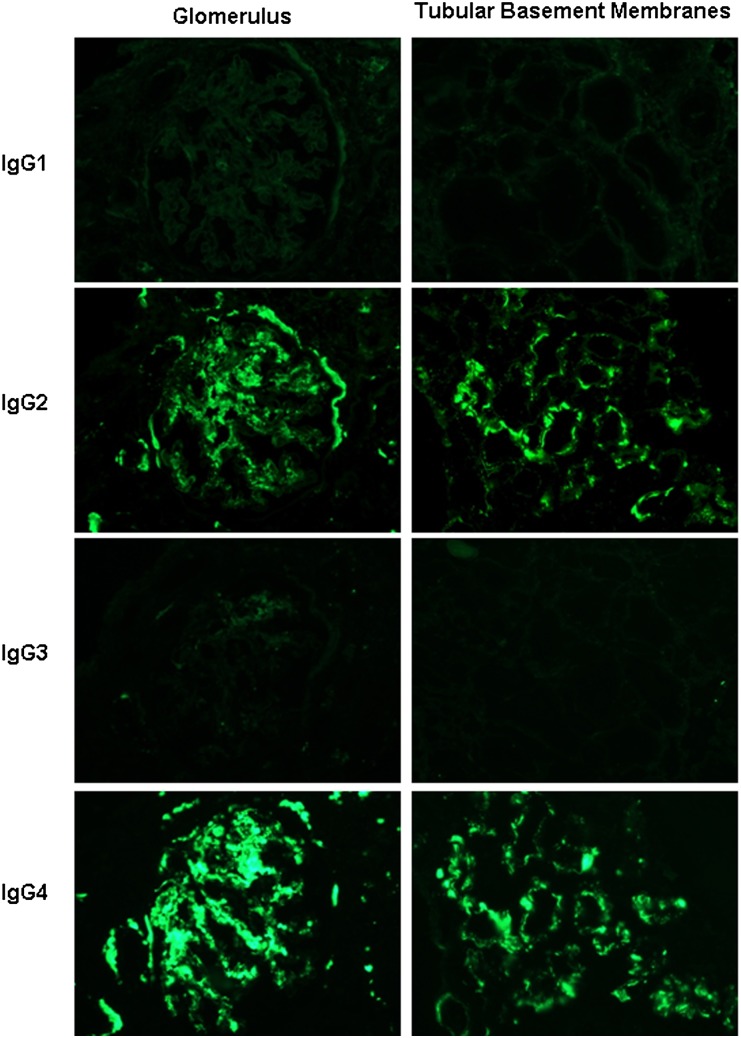
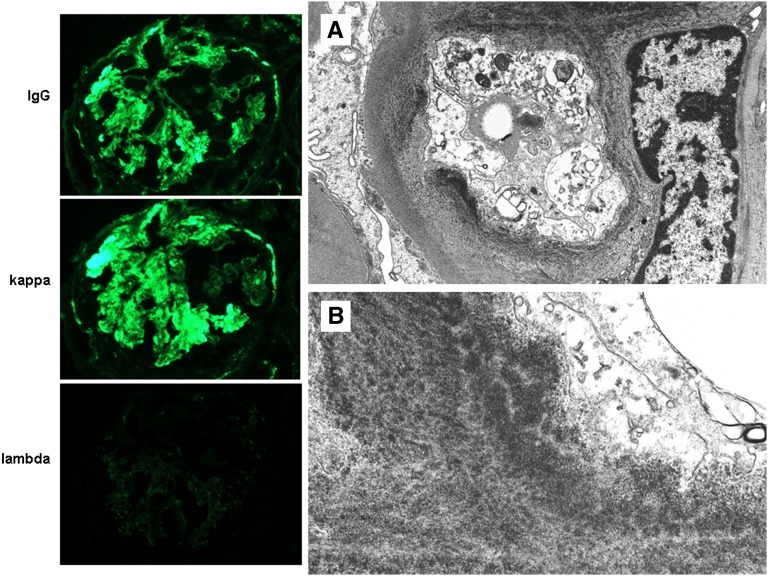
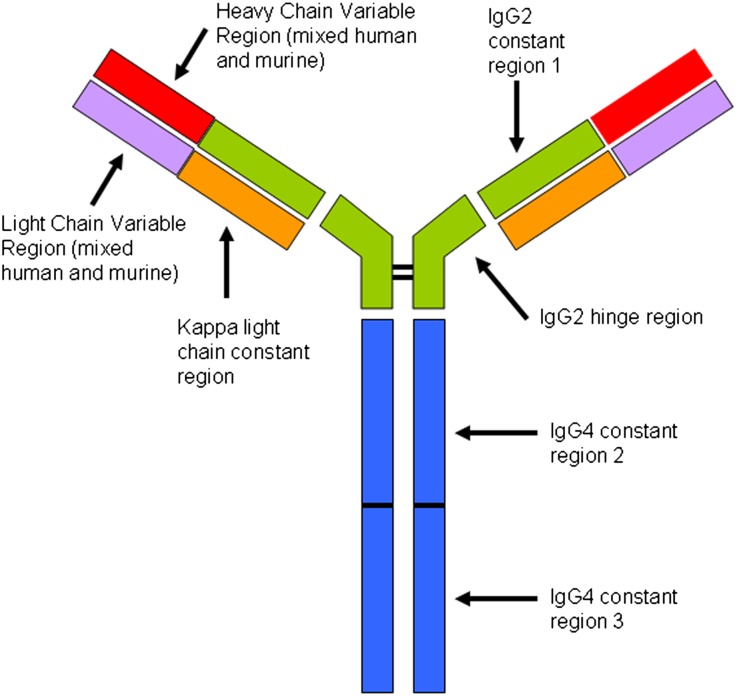
Eculizumab might benefit C3 glomerulopathies mediated by dysregulation of the alternative complement pathway. Here, we report renal biopsy findings before and after eculizumab therapy in three patients with dense deposit disease and two with C3 GN. All pretreatment biopsies had glomerular and tubular basement membrane deposits that stained exclusively for C3 without significant Ig. After 1 year of therapy, there was reduction in active glomerular proliferation and neutrophil infiltration in three of five patients, consistent with effective C5 blockade, which prevents production of chemotactin C5a. One individual with mild mesangial disease had no significant change in activity or chronicity. One patient exhibited persistent activity and worsening chronicity despite therapy. Immunofluorescence showed no significant reduction in C3 or C5b-9, and electron microscopy revealed persistent deposits in all cases, suggesting a long t(1/2) of C5b-9 in extracellular matrix. Normal renal biopsies stained positive for C5b-9 in glomeruli, tubular basement membranes, and vessel walls, albeit at lower intensity than in C3 glomerulopathy. This indication of physiologic levels of C5b-9 activation in normal kidney potentially explains the localization of deposits in patients with dysregulation of the alternative complement pathway. All post-treatment biopsies showed de novo monoclonal staining for IgG-κ in the same distribution as C3 and C5b-9, mimicking monoclonal Ig deposition disease (MIDD). Staining of the γ heavy chain was restricted to the IgG2 and IgG4 subclasses, suggesting the binding of monoclonal eculizumab to C5 in renal tissues. The long-term effects of this apparent drug-tissue interaction are unknown.
Figures

References
-
- Fakhouri F, Frémeaux-Bacchi V, Noël LH, Cook HT, Pickering MC: C3 glomerulopathy: A new classification. Nat Rev Nephrol 6: 494–499, 2010 - PubMed
-
- Servais A, Frémeaux-Bacchi V, Lequintrec M, Salomon R, Blouin J, Knebelmann B, Grünfeld JP, Lesavre P, Noël LH, Fakhouri F: Primary glomerulonephritis with isolated C3 deposits: A new entity which shares common genetic risk factors with haemolytic uraemic syndrome. J Med Genet 44: 193–199, 2007 - PMC - PubMed
-
- D'Agati VD, Jennette JC, Silva FG: Non-Neoplastic Kidney Diseases, Washington, DC, American Registry of Pathology, 2005, pp 250–255
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
