

Sagittal balance correction of idiopathic scoliosis using the in situ contouring technique
- PMID: 22678557
- PMCID: PMC3463684
- DOI: 10.1007/s00586-012-2356-2
Sagittal balance correction of idiopathic scoliosis using the in situ contouring technique
Abstract
Purpose: Idiopathic scoliosis can lead to sagittal imbalance. The relationship between thoracic hyper- and hypo-kyphotic segments, vertebral rotation and coronal curve was determined. The effect of segmental sagittal correction by in situ contouring was analyzed.
Methods: Pre- and post-operative radiographs of 54 scoliosis patients (Lenke 1 and 3) were analyzed at 8 years follow-up. Cobb angles and vertebral rotation were determined. Sagittal measurements were: kyphosis T4-T12, T4-T8 and T9-T12, lordosis L1-S1, T12-L2 and L3-S1, pelvic incidence, pelvic tilt, sacral slope, T1 and T9 tilt.
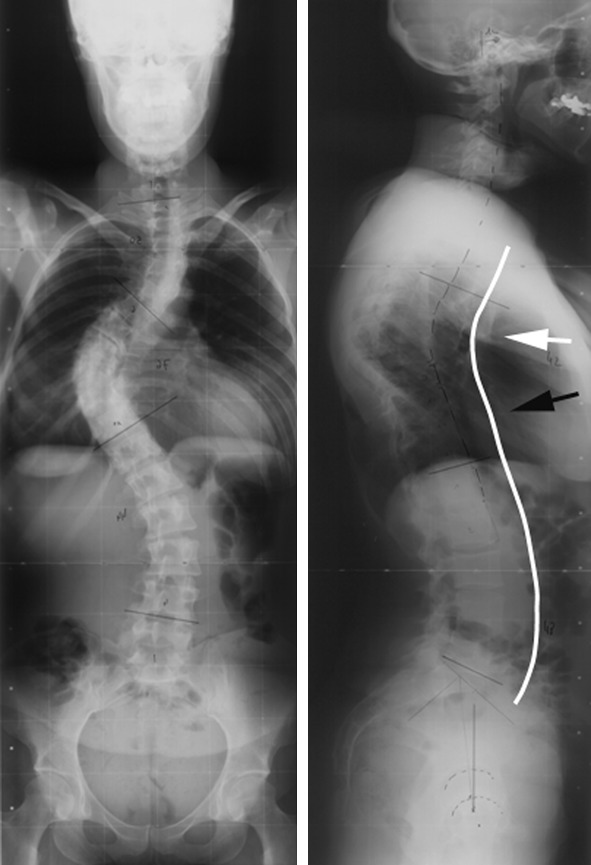
Results: Thoracic and lumbar curves were significantly reduced (p = 0.0001). Spino-pelvic parameters, T1 and T9 tilt were not modified. The global T4-T12 kyphosis decreased by 2.1° on average (p = 0.066). Segmental analysis evidenced a significant decrease of T4-T8 hyperkyphosis by 6.6° (p = 0.0001) and an increase of segmental hypokyphosis T9-T12 by 5.0° (p = 0.0001). Maximal vertebral rotation was located at T7, T8 or T9 and correlated (r = 0.422) with the cranial level of the hypokyphotic zone (p = 0.003). This vertebra or its adjacent levels corresponded to the coronal apex in 79.6 % of thoracic curves.
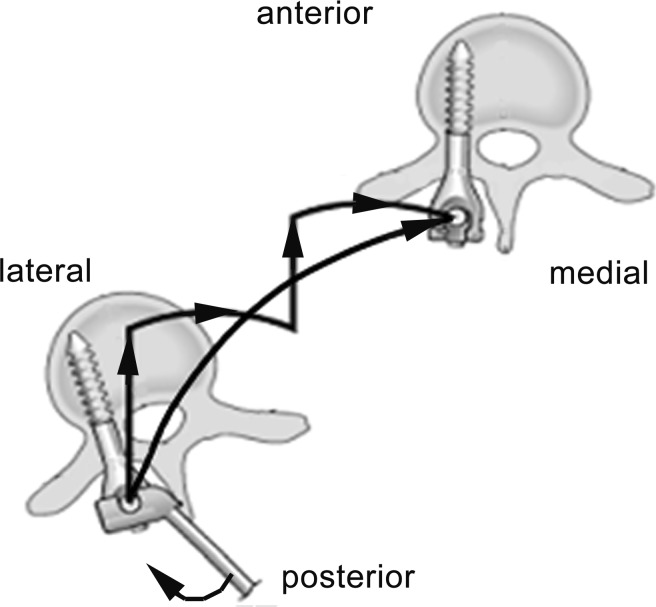
Conclusions: Lenke 1 and 3 curves can show normal global kyphosis, divided in cranial hyperkyphosis and caudal hypokyphosis. The cranial end of hypokyphosis corresponds to maximal rotation. These vertebrae have most migrated anteriorly and laterally. The sagittal apex between segmental hypo- and hyper-kyphosis corresponds to the coronal thoracic apex. A segmental sagittal imbalance correction is achieved by in situ contouring. The concept of segmental imbalance is useful when determining the levels on which surgical detorsion may be focused.
Figures




Similar articles
-
Thoracic sagittal plane variations between patients with thoracic adolescent idiopathic scoliosis and healthy adolescents.Eur Spine J. 2016 Oct;25(10):3095-3103. doi: 10.1007/s00586-016-4400-0. Epub 2016 Jan 28. Eur Spine J. 2016. PMID: 26821145
-
Cervical sagittal alignment in idiopathic scoliosis treated by posterior instrumentation and in situ bending.Spine (Phila Pa 1976). 2015 Apr 1;40(7):E419-27. doi: 10.1097/BRS.0000000000000767. Spine (Phila Pa 1976). 2015. PMID: 25902150
-
Cervical sagittal alignment in adult hyperkyphosis treated by posterior instrumentation and in situ bending.Orthop Traumatol Surg Res. 2017 Feb;103(1):53-59. doi: 10.1016/j.otsr.2016.10.003. Epub 2016 Nov 23. Orthop Traumatol Surg Res. 2017. PMID: 27889355
-
Pre- and post-operative sagittal balance in idiopathic scoliosis: a comparison over the ages of two cohorts of 132 adolescents and 52 adults.Eur Spine J. 2013 Mar;22 Suppl 2(Suppl 2):S203-15. doi: 10.1007/s00586-012-2571-x. Epub 2012 Nov 28. Eur Spine J. 2013. PMID: 23188161 Free PMC article.
-
Sagittal plane correction in idiopathic scoliosis.Spine (Phila Pa 1976). 2002 Apr 1;27(7):754-60. doi: 10.1097/00007632-200204010-00013. Spine (Phila Pa 1976). 2002. PMID: 11923669
Cited by
-
Thoracic sagittal plane variations between patients with thoracic adolescent idiopathic scoliosis and healthy adolescents.Eur Spine J. 2016 Oct;25(10):3095-3103. doi: 10.1007/s00586-016-4400-0. Epub 2016 Jan 28. Eur Spine J. 2016. PMID: 26821145
-
Maximal Axial Vertebral Rotation in Adolescent Idiopathic Scoliosis: Is the Apical Vertebra the Most Rotated?Global Spine J. 2022 Mar;12(2):244-248. doi: 10.1177/2192568220948830. Epub 2020 Sep 16. Global Spine J. 2022. PMID: 32935571 Free PMC article.
-
Choice of Rods in Surgical Treatment of Adolescent Idiopathic Scoliosis: What Are the Clinical Implications of Biomechanical Properties? - A Review of the Literature.Neurospine. 2018 Jun;15(2):123-130. doi: 10.14245/ns.1836050.025. Epub 2018 Jun 19. Neurospine. 2018. PMID: 29991241 Free PMC article.
-
Percutaneous three column osteotomy for kyphotic deformity correction in congenital kyphosis.Eur Spine J. 2013 Sep;22(9):2139-41. doi: 10.1007/s00586-013-2958-3. Eur Spine J. 2013. PMID: 23996007 Free PMC article. No abstract available.
-
Use of a novel corrective device for correction of deformities in adolescent idiopathic scoliosis.Ir J Med Sci. 2020 Feb;189(1):203-210. doi: 10.1007/s11845-019-02031-6. Epub 2019 May 18. Ir J Med Sci. 2020. PMID: 31104287
References
-
- Graf H, Hecquet J, Dubousset J. Approche tridimensionnelle des déformations rachidiennes. Application à l’étude des scolioses infantiles. Rev Chir Orthop Reparatrice Appar Mot. 1983;69:407–416. - PubMed
-
- Cotrel Y, Dubousset J, Guillaumat M. New universal instrumentation in spinal surgery. Clin Orthop Relat Res. 1988;227:10–23. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
