

Follow-up of coiled intracranial aneurysms: comparison of 3D time-of-flight MR angiography at 3T and 1.5T in a large prospective series
- PMID: 22678846
- PMCID: PMC7965594
- DOI: 10.3174/ajnr.A3124
Follow-up of coiled intracranial aneurysms: comparison of 3D time-of-flight MR angiography at 3T and 1.5T in a large prospective series
Abstract
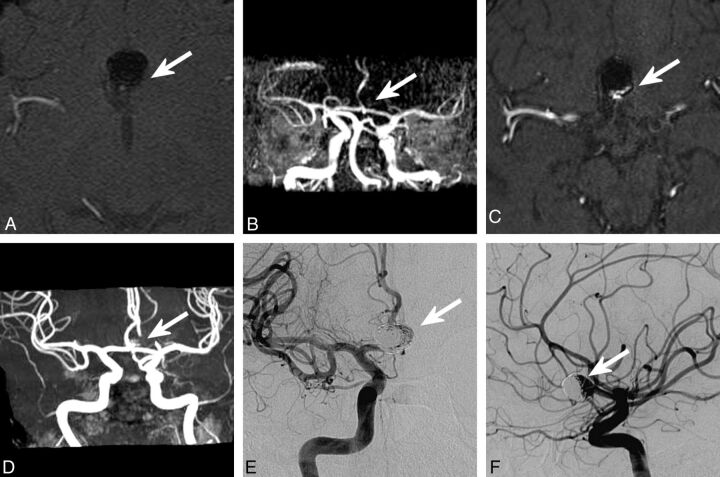
Background and purpose: Our aim was to compare 3D TOF-MRA sequences at 3T and 1.5T in the follow-up of coiled aneurysms. The follow-up of coiled intracranial aneurysms is mandatory to depict potential recanalization. 3D-TOF MRA is an appropriate tool for this purpose.
Materials and methods: DSA and 3D TOF-MRA at 1.5T and 3T were performed in a prospective series of 126 aneurysms in 96 patients (58 women, 38 men; age, 25-75 years; mean, 51.3 ± 11.3 years). DSA was the reference standard to which the accuracy of 3D TOF-MRA was compared. The quality of aneurysm occlusion was assessed independently and anonymously by a core lab by using a 3-grade scale (total occlusion, neck remnant, and aneurysm remnant). Adequate occlusion was defined as total occlusion or neck remnant and used in a 2-grade scale: adequate occlusion/aneurysm remnant.
Results: With DSA, total occlusion was depicted in 58 aneurysms (46.0%); neck remnant, in 33 aneurysms (26.2%); and aneurysm remnant, in 35 aneurysms (27.8%). Adequate occlusion was seen in 91 cases (72.2%). A remnant (aneurysm or neck) was depicted in 68 cases (54.0%). For the 3 imaging techniques and regardless of scale used, the interobserver agreement was always greater at 3T than at 1.5T. SE and NPV for the prediction of aneurysm remnant versus adequate occlusion were higher at 3T than at 1.5T (SE 3T, 0.74; SE 1.5T, 0.54; NPV 3T, 0.90; NPV 1.5T, 0.85).
Conclusions: In this large prospective series of patients, 3D TOF-MRA was superior at 3T to 1.5T for the evaluation of coiled intracranial aneurysms.
Conflict of interest statement
The authors declare that they have no conflict of interest with the topic of the manuscript.
Figures
Similar articles
-
Contrast-Enhanced and Time-of-Flight MRA at 3T Compared with DSA for the Follow-Up of Intracranial Aneurysms Treated with the WEB Device.AJNR Am J Neuroradiol. 2016 Sep;37(9):1684-9. doi: 10.3174/ajnr.A4791. Epub 2016 Apr 21. AJNR Am J Neuroradiol. 2016. PMID: 27102311 Free PMC article.
-
Follow-up of coiled intracranial aneurysms: comparison of 3D time-of-flight and contrast-enhanced magnetic resonance angiography at 3T in a large, prospective series.Eur Radiol. 2012 Oct;22(10):2255-63. doi: 10.1007/s00330-012-2466-6. Epub 2012 May 9. Eur Radiol. 2012. PMID: 22569997
-
A prospective trial of 3T and 1.5T time-of-flight and contrast-enhanced MR angiography in the follow-up of coiled intracranial aneurysms.AJNR Am J Neuroradiol. 2010 May;31(5):912-8. doi: 10.3174/ajnr.A1932. Epub 2009 Dec 17. AJNR Am J Neuroradiol. 2010. PMID: 20019107 Free PMC article. Clinical Trial.
-
MRA versus DSA for the follow-up imaging of intracranial aneurysms treated using endovascular techniques: a meta-analysis.J Neurointerv Surg. 2019 Oct;11(10):1009-1014. doi: 10.1136/neurintsurg-2019-014936. Epub 2019 May 2. J Neurointerv Surg. 2019. PMID: 31048457 Review.
-
Diagnosing flow residuals in coiled cerebral aneurysms by MR angiography: meta-analysis.J Neurol. 2014 Apr;261(4):655-62. doi: 10.1007/s00415-013-7053-5. Epub 2013 Jul 28. J Neurol. 2014. PMID: 23893001 Free PMC article. Review.
Cited by
-
WEB-DL Endovascular Treatment of Wide-Neck Bifurcation Aneurysms: Long-Term Results in a European Series.AJNR Am J Neuroradiol. 2015 Dec;36(12):2314-9. doi: 10.3174/ajnr.A4445. Epub 2015 Jul 30. AJNR Am J Neuroradiol. 2015. PMID: 26228882 Free PMC article.
-
Contrast-Enhanced and Time-of-Flight MRA at 3T Compared with DSA for the Follow-Up of Intracranial Aneurysms Treated with the WEB Device.AJNR Am J Neuroradiol. 2016 Sep;37(9):1684-9. doi: 10.3174/ajnr.A4791. Epub 2016 Apr 21. AJNR Am J Neuroradiol. 2016. PMID: 27102311 Free PMC article.
-
Usefulness of Craniograms in Discriminating Coiled Intracranial Aneurysms Requiring Retreatment.Neurol Med Chir (Tokyo). 2022 Mar 15;62(3):118-124. doi: 10.2176/nmc.oa.2021-0225. Epub 2021 Dec 8. Neurol Med Chir (Tokyo). 2022. PMID: 34880195 Free PMC article.
-
Follow-Up Assessment of Intracranial Aneurysms Treated with Endovascular Coiling: Comparison of Compressed Sensing and Parallel Imaging Time-of-Flight Magnetic Resonance Angiography.Tomography. 2022 Jun 18;8(3):1608-1617. doi: 10.3390/tomography8030133. Tomography. 2022. PMID: 35736881 Free PMC article.
-
Imaging follow-up strategy after endovascular treatment of Intracranial aneurysms: A literature review and guideline recommendations.J Cerebrovasc Endovasc Neurosurg. 2024 Mar;26(1):1-10. doi: 10.7461/jcen.2024.E2023.08.008. Epub 2024 Mar 25. J Cerebrovasc Endovasc Neurosurg. 2024. PMID: 38523549 Free PMC article.
References
-
- Molyneux AJ, Kerr RSC, Stratton I, et al. . International Subarachnoid Aneurysm Trial (ISAT) of neurosurgical clipping versus endovascular coiling in 2143 patients with ruptured intracranial aneurysms: a randomised trial. Lancet 2002;360:1262–63 - PubMed
-
- Pierot L, Spelle L, Vitry F, et al. . Immediate clinical outcome of patients harboring unruptured intracranial aneurysms treated by endovascular approach: results of the ATENA study. Stroke 2008;39:2497–504 - PubMed
-
- Ferns SP, Sprengers MES, von Rooij WJ, et al. . Coiling of intracranial aneurysms: a systematic review on initial occlusion and reopening and retreatment rates. Stroke 2009;40:e523–29 - PubMed
-
- Kaufmann TJ, Huston J, Mandrekar JN, et al. . Complications of diagnostic cerebral angiography: evaluation of 19,826 consecutive patients. Radiology 2007;243:812–19 - PubMed
-
- Boulin A, Pierot L. Follow-up of intracranial aneurysms treated with detachable coils: comparison of gadolinium 3D time-of-flight MR angiography and digital subtraction angiography. Radiology 2001;219:108–13 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous