

Permanent haemichorea associated with transient hyperglycemia
- PMID: 22679165
- PMCID: PMC3189650
- DOI: 10.1136/bcr.08.2011.4641
Permanent haemichorea associated with transient hyperglycemia
Abstract
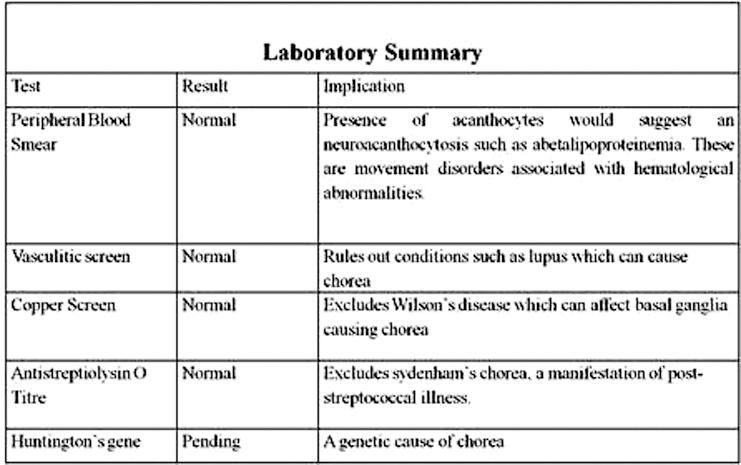
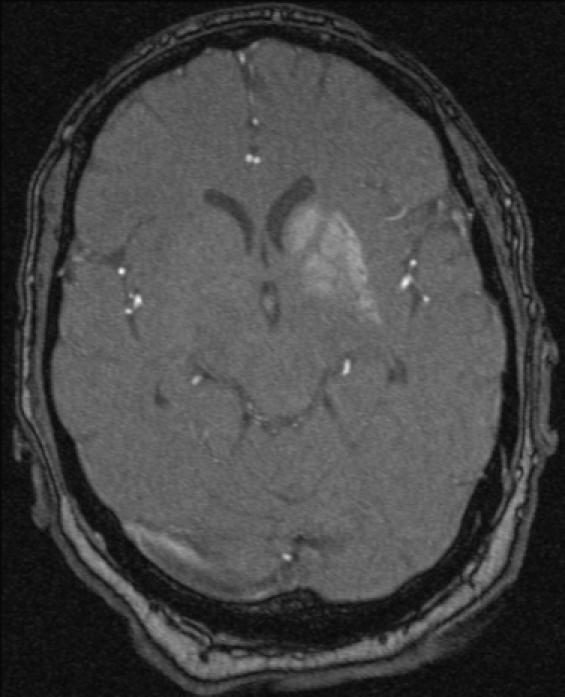
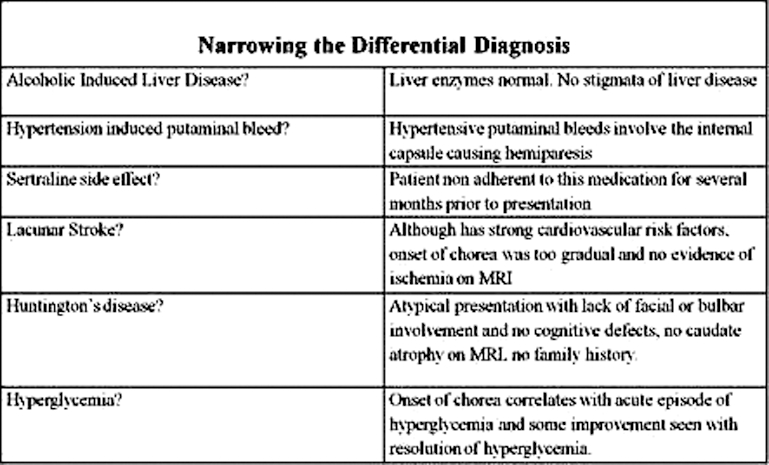
Hyperglycemia is associated with several common neurological syndromes. Chorea, however, is a rare association that has only been documented in the literature recently. The triad of chorea, non-ketotic hyperglycemia and a high signal basal ganglia lesion on the T1 weighted brain MRI (C-H-BG) is considered to be a unique syndrome. C-H-BG refers to the onset of chorea during or shortly after (days to weeks) an episode of non-ketotic hyperglycemia. There is usually a high signal lesion in the basal ganglia on T1 weighted brain MRI that corresponds to the location of the chorea. Most case reports of C-H-BG have been described in Asians. C-H-BG is considered to be a benign condition in which the clinical and MRI signs resolve quickly upon correction of blood glucose levels. Here, the authors describe a case of C-H-BG in a middle aged Caucasian in whom the chorea did not resolve with improved glycemic control.
Conflict of interest statement
Figures
References
-
- Cardoso F, Seppi K, Mair KJ, et al. Seminar on choreas. Lancet Neurol 2006;5:589–602 - PubMed
-
- Iwata A, Koike F, Arasaki K, et al. Blood brain barrier destruction in hyperglycemic chorea in a patient with poorly controlled diabetes. J Neurol Sci 1999;163:90–3 - PubMed
-
- Oh SH, Lee KY, Im JH, et al. Chorea associated with non-ketotic hyperglycemia and hyperintensity basal ganglia lesion on T1-weighted brain MRI study: a meta-analysis of 53 cases including four present cases. J Neurol Sci 2002;200:57–62 - PubMed
-
- Hsu JL, Wang HC, Hsu WC. Hyperglycemia-induced unilateral basal ganglion lesions with and without hemichorea. A PET study. J Neurol 2004;251:1486–90 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical