

Severe intracranial haemorrhage in neonatal alloimmune thrombocytopenia
- PMID: 22679192
- PMCID: PMC3176384
- DOI: 10.1136/bcr.07.2011.4563
Severe intracranial haemorrhage in neonatal alloimmune thrombocytopenia
Abstract
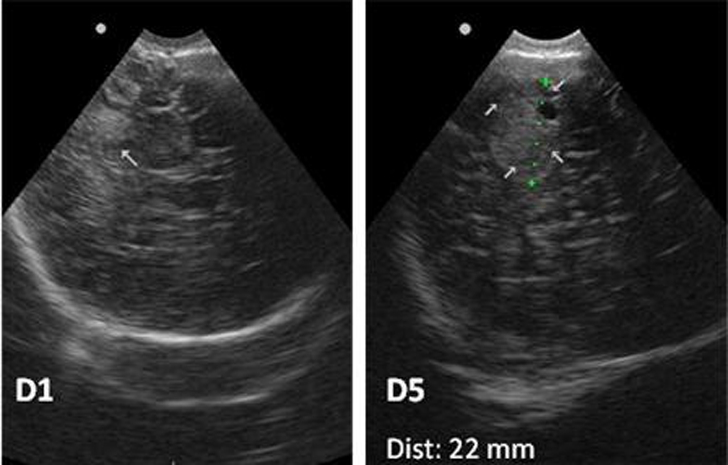
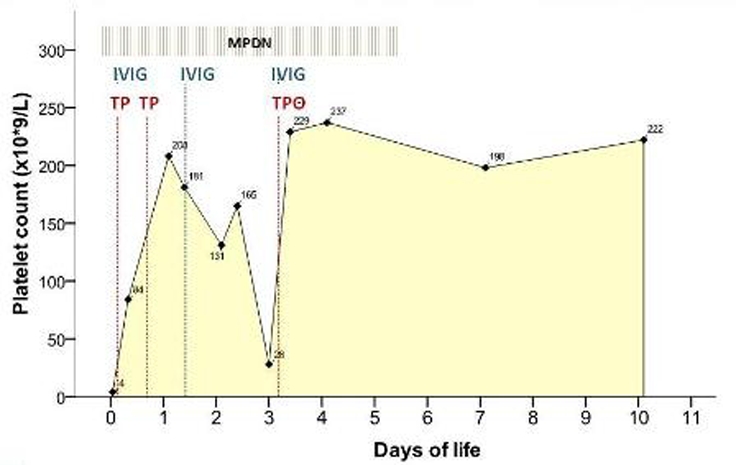
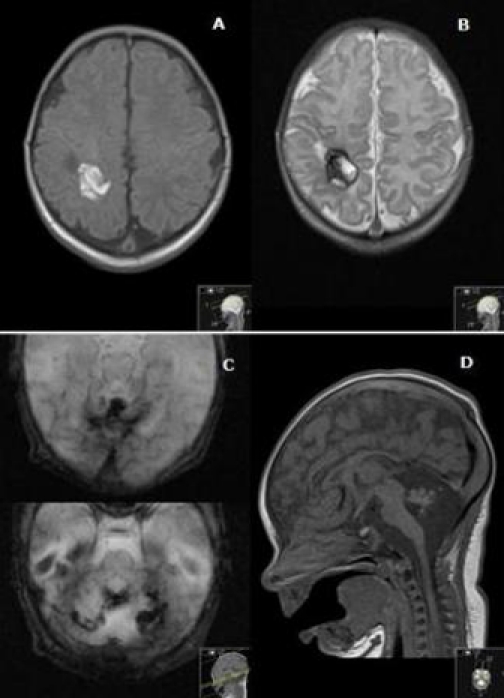
Neonatal alloimmune thrombocytopenia is a rare (1/1000-5000 births) life-threatening disorder, caused by fetomaternal incompatibility for a fetal human platelet alloantigen inherited from the father, with production of maternal alloantibodies against fetal platelets, leading to severe thrombocytopenia and potential bleeding. Intracranial haemorrhage is the most feared complication. This report presents the case of a term newborn infant, born from caesarean section after a normal pregnancy, presenting signs of skin bleeding with different ages. Obstetric history included a previous spontaneous abortion after amniocentesis. Severe thrombocytopenia (4×10(9)/l platelets) was found and brain ultrasound showed multiple intracranial haemorrhages. Human platelet antigen (HPA) phenotyping showed maternal negative HPA-1a and paternal positive HPA-1a platelets. Strongly positive anti-HPA-1a and weakly positive anti-human leukocyte antigen class I alloantibodies were found in the mother. Multiple platelet transfusions, intravenous immunoglobulin and corticosteroid were given but favourable response was accomplished only after a compatible platelet transfusion. Brain MRI showed multiple subacute and chronic haemorrhages.
Conflict of interest statement
Figures

References
-
- Fernandes CJ. Neonatal Thrombocytopenia. http://www.uptodate.com/contents/neonatal-thrombocytopenia (accessed 15 Feb 2011).
-
- Blanchsette VS, Johnson J, Rand M. The management of alloimmune neonatal thrombocytopenia. Baillieres Best Pract Res Clin Haematol 2000;13:365–90 - PubMed
-
- Berkowitz RL, Bussel JB, McFarland JG. Alloimmune thrombocytopenia: state of the art 2006. Am J Obstet Gynecol 2006;195:907–13 - PubMed
-
- Arnold DM, Smith JW, Kelton JG. Diagnosis and management of neonatal alloimmune thrombocytopenia. Transfus Med Rev 2008;22:255–67 - PubMed
-
- Mendes LR, Ferrão A, Malcata C, et al. trombocitopénia neonatal aloimune –apresentação clínica tardia. Acta Pediatr Port 2006;7:27–9
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources