

The ability of synovitis to predict structural damage in rheumatoid arthritis: a comparative study between clinical examination and ultrasound
- PMID: 22679298
- PMCID: PMC3618684
- DOI: 10.1136/annrheumdis-2012-201469
The ability of synovitis to predict structural damage in rheumatoid arthritis: a comparative study between clinical examination and ultrasound
Erratum in
- Ann Rheum Dis. 2013 Jul;72(7):1270. Etcheparre, Frederic [corrected to Etchepare, Fabien]
Abstract
Objectives: To evaluate synovitis (clinical vs ultrasound (US)) to predict structural progression in rheumatoid arthritis (RA).
Methods: Patients with RA.
Study design: Prospective, 2-year follow-up.
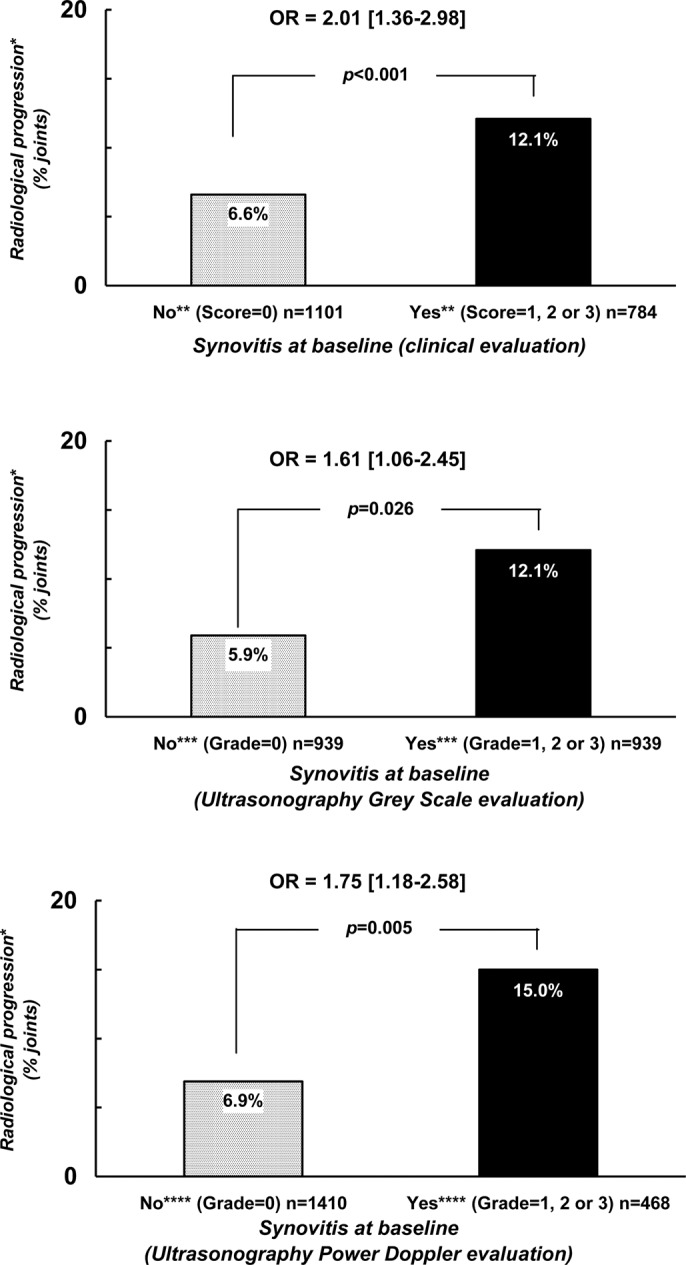
Data collected: Synovitis (32 joints (2 wrists, 10 metacarpophalangeal, 10 proximal interphalangeal, 10 metatarsophalangeal)) at baseline and after 4 months of therapy by clinical, US grey scale (GS-US) and power doppler (PD-US); x-rays at baseline and at year 2.
Analysis: Measures of association (OR) were tested between structural deterioration and the presence of baseline synovitis, or its persistence, after 4 months of therapy using generalised estimating equation analysis.
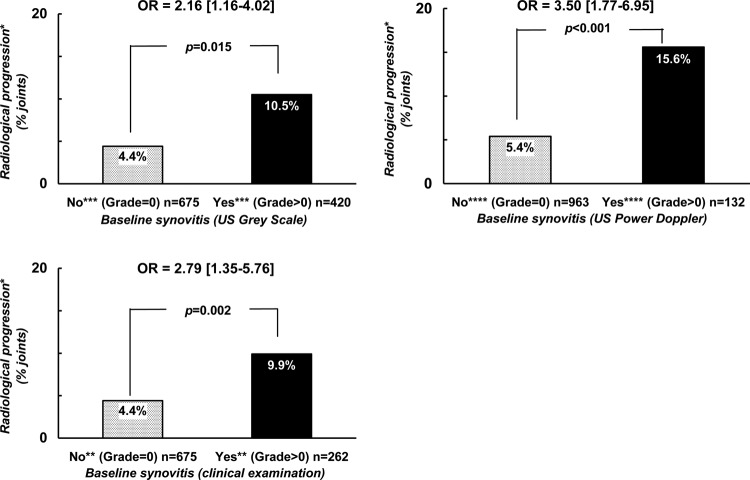
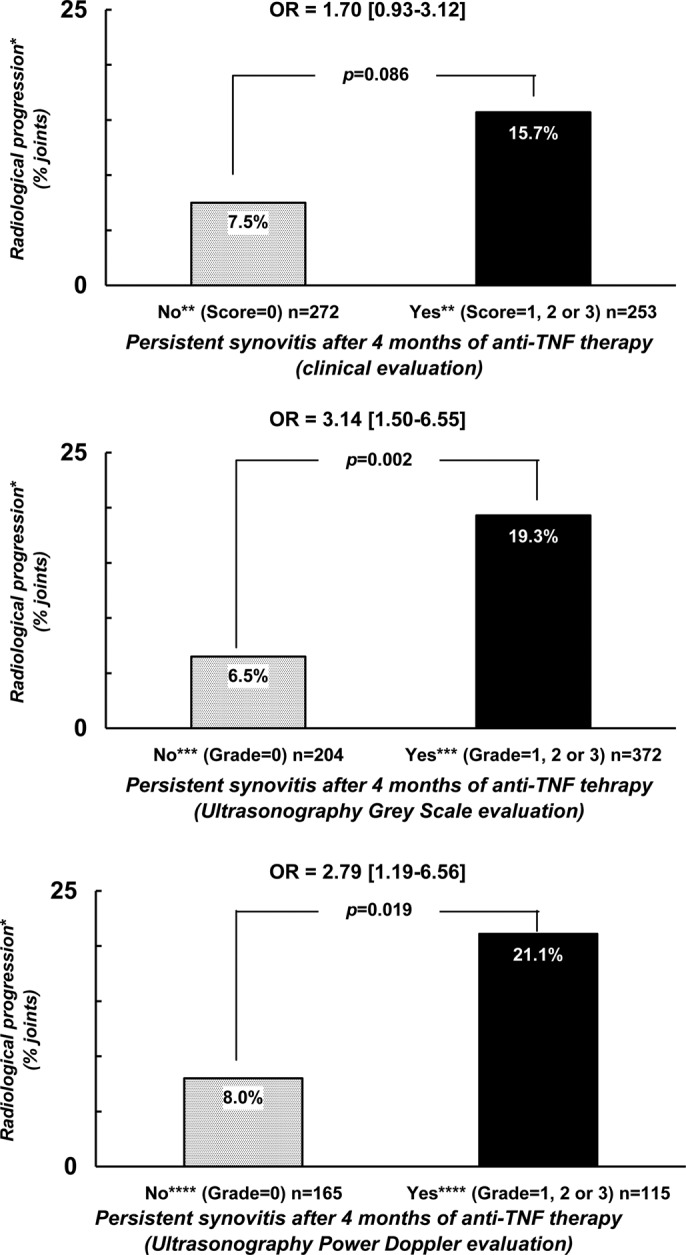
Results: Structural deterioration was observed in 9% of the 1888 evaluated joints in 59 patients. Baseline synovitis increased the risk of structural progression: OR=2.01 (1.36-2.98) p<0.001 versus 1.61 (1.06-2.45) p=0.026 versus 1.75 (1.18-2.58) p=0.005 for the clinical versus US-GS versus US-PD evaluation, respectively. In the joints with normal baseline examination (clinical or US), an increased probability for structural progression in the presence of synovitis for the other modality was also observed (OR=2.16 (1.16-4.02) p=0.015 and 3.50 (1.77-6.95) p<0.001 for US-GS and US-PD and 2.79 (1.35-5.76) p=0.002) for clinical examination. Persistent (vs disappearance) synovitis after 4 months of therapy was also predictive of subsequent structural progression.
Conclusions: This study confirms the validity of synovitis for predicting subsequent structural deterioration irrespective of the modality of examination of joints, but also suggests that both clinical and ultrasonographic examinations may be relevant to optimally evaluate the risk of subsequent structural deterioration.
Conflict of interest statement
Figures
References
-
- Drossaers-Bakker KW, de Buck M, van Zeben D, et al. Long-term course and outcome of functional capacity in rheumatoid arthritis: the effect of disease activity and radiologic damage over time. Arthritis Rheum 1999;42:1854–60 - PubMed
-
- Aletaha D, Smolen J, Ward MM. Measuring function in rheumatoid arthritis: Identifying reversible and irreversible components. Arthritis Rheum 2006;54:2784–92 - PubMed
-
- van Leeuwen MA, van der Heijde DM, van Rijswijk MH, et al. Interrelationship of outcome measures and process variables in early rheumatoid arthritis. A comparison of radiologic damage, physical disability, joint counts, and acute phase reactants. J Rheumatol 1994;21:425–9 - PubMed
