

Implementation of ICD-10 in Canada: how has it impacted coded hospital discharge data?
- PMID: 22682405
- PMCID: PMC3411494
- DOI: 10.1186/1472-6963-12-149
Implementation of ICD-10 in Canada: how has it impacted coded hospital discharge data?
Abstract
Background: The purpose of this study was to assess whether or not the change in coding classification had an impact on diagnosis and comorbidity coding in hospital discharge data across Canadian provinces.
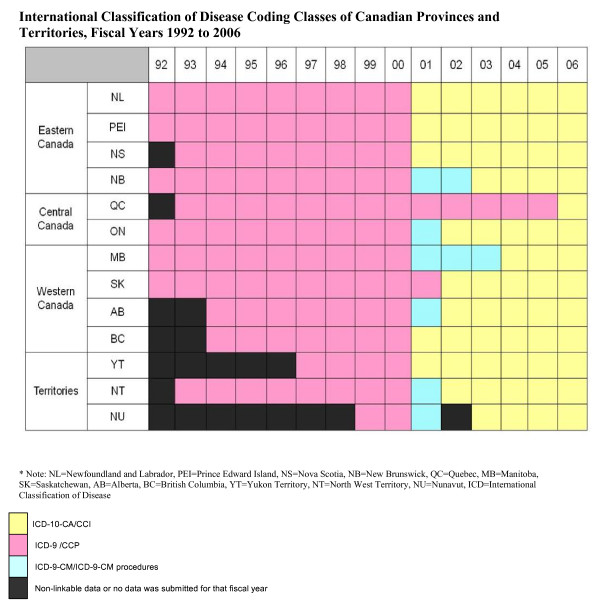
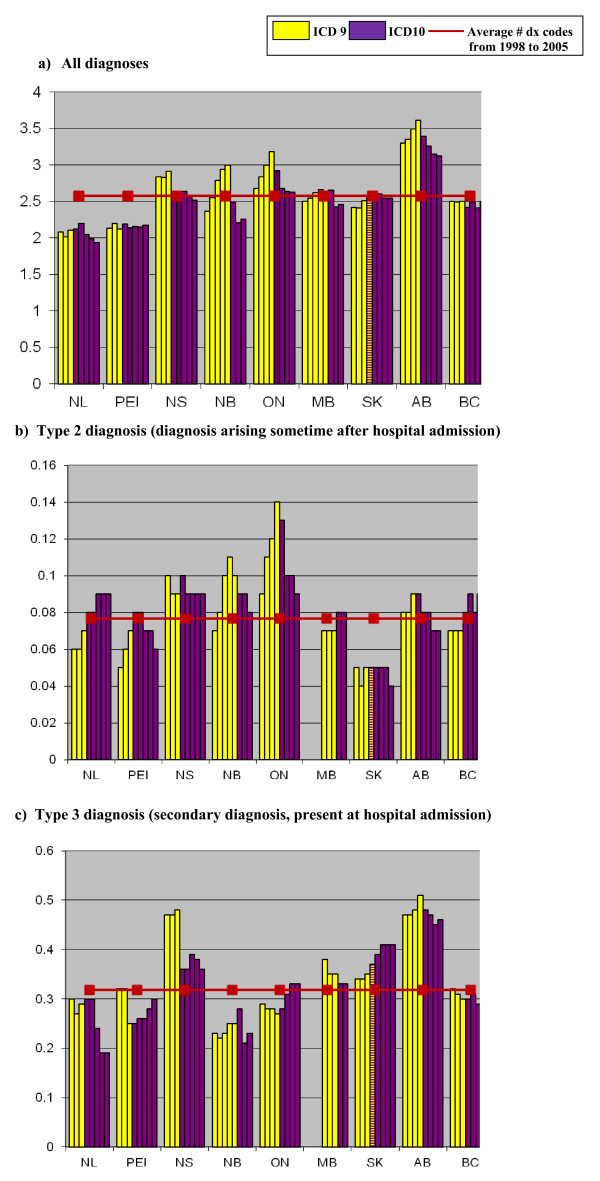
Methods: This study examined eight years (fiscal years 1998 to 2005) of hospital records from the Hospital Person-Oriented Information database (HPOI) derived from the Canadian national Discharge Abstract Database. The average number of coded diagnoses per hospital visit was examined from 1998 to 2005 for provinces that switched from International Classifications of Disease 9(th) version (ICD-9-CM) to ICD-10-CA during this period. The average numbers of type 2 and 3 diagnoses were also described. The prevalence of the Charlson comorbidities and distribution of the Charlson score one year before and one year after ICD-10 implementation for each of the 9 provinces was examined. The prevalence of at least one of the seventeen Charlson comorbidities one year before and one year after ICD-10 implementation were described by hospital characteristics (teaching/non-teaching, urban/rural, volume of patients).
Results: Nine Canadian provinces switched from ICD-9-CM to ICD-I0-CA over a 6 year period starting in 2001. The average number of diagnoses coded per hospital visit for all code types over the study period was 2.58. After implementation of ICD-10-CA a decrease in the number of diagnoses coded was found in four provinces whereas the number of diagnoses coded in the other five provinces remained similar. The prevalence of at least one of the seventeen Charlson conditions remained relatively stable after ICD-10 was implemented, as did the distribution of the Charlson score. When stratified by hospital characteristics, the prevalence of at least one Charlson condition decreased after ICD-10-CA implementation, particularly for low volume hospitals.
Conclusion: In conclusion, implementation of ICD-10-CA in Canadian provinces did not substantially change coding practices, but there was some coding variation in the average number of diagnoses per hospital visit across provinces.
Figures
References
-
- Feasby TE, Quan H, Ghali WA. Provincial carotid endarterectomy outcomes. Can J Neurol Sci. 2002;29:333–336. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
