

Delirium in hospitalized patients: implications of current evidence on clinical practice and future avenues for research--a systematic evidence review
- PMID: 22684893
- PMCID: PMC3640527
- DOI: 10.1002/jhm.1949
Delirium in hospitalized patients: implications of current evidence on clinical practice and future avenues for research--a systematic evidence review
Abstract
Background: Despite the significant burden of delirium among hospitalized adults, critical appraisal of systematic data on delirium diagnosis, pathophysiology, treatment, prevention, and outcomes is lacking.
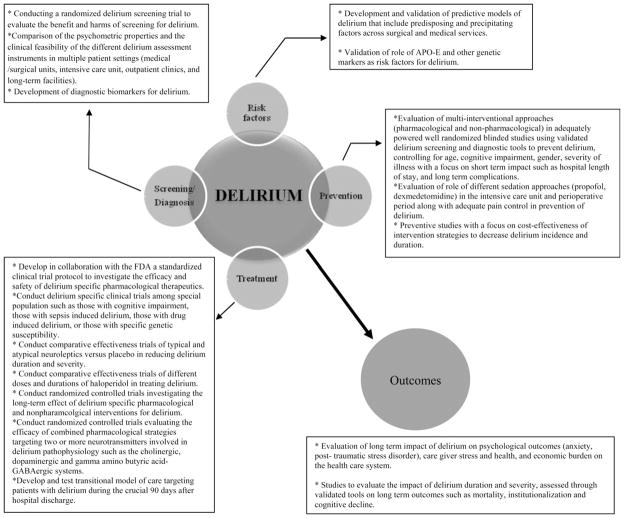
Purpose: To provide evidence-based recommendations for delirium care to practitioners, and identify gaps in delirium research.
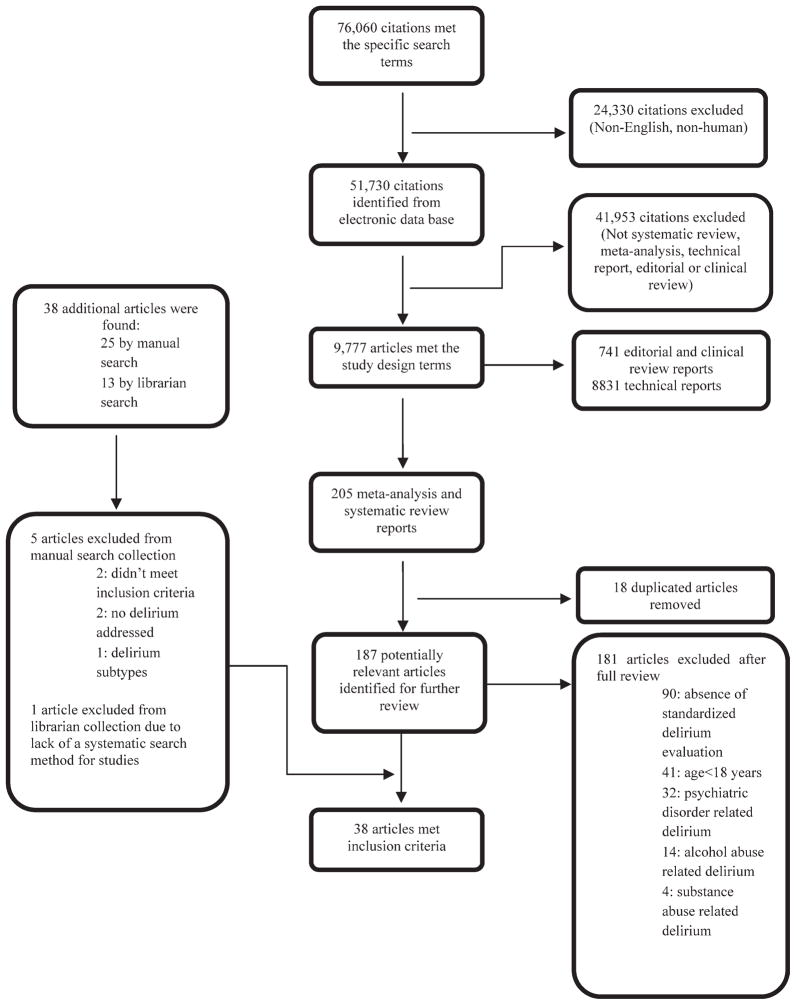
Data sources: Medline, PubMed, the Cochrane Library, and the Cumulative Index to Nursing and Allied Health Literature (CINAHL) information systems from January 1966 to April 2011.
Study selection: All published systematic evidence reviews (SERs) on delirium were evaluated.
Data extraction: Three reviewers independently extracted the data regarding delirium risk factors, diagnosis, prevention, treatment, and outcomes, and critically appraised each SER as good, fair, or poor using the United States Preventive Services Task Force criteria.
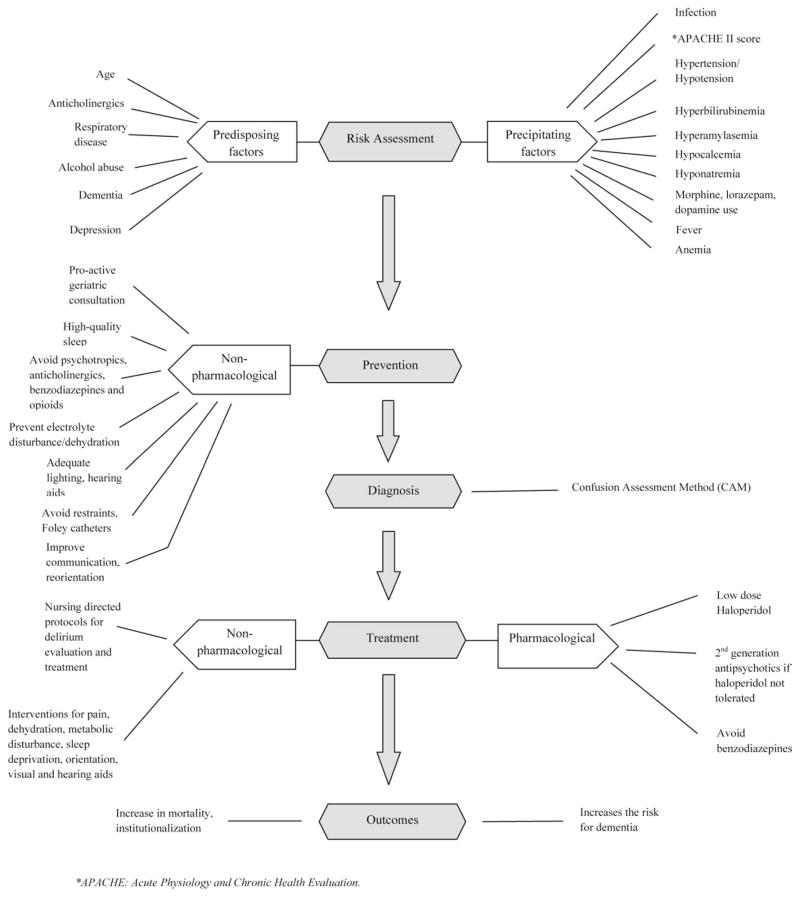
Data synthesis: Twenty-two SERs graded as good or fair provided the data. Age, cognitive impairment, depression, anticholinergic drugs, and lorazepam use were associated with an increased risk for developing delirium. The Confusion Assessment Method (CAM) is reliable for delirium diagnosis outside of the intensive care unit. Multicomponent nonpharmacological interventions are effective in reducing delirium incidence in elderly medical patients. Low-dose haloperidol has similar efficacy as atypical antipsychotics for treating delirium. Delirium is associated with poor outcomes independent of age, severity of illness, or dementia.
Conclusion: Delirium is an acute, preventable medical condition with short- and long-term negative effects on a patient's cognitive and functional states.
Copyright © 2012 Society of Hospital Medicine.
Figures
References
-
- Inouye SK, Van Dyck CH, Alessi CA, Balkin S, Siegal AP, Horwitz RI. Clarifying delirium: the confusion assessment method. A new method for detection of delirium. Ann Intern Med. 1990;113(12):941–948. - PubMed
-
- Trzepacz PT, Sclabassi RJ, van Theil DH. Delirium; a subcortical phenomenon? J Neuropsychiatry Clin Neurosci. 1989;1(3):283–290. - PubMed
-
- Lin SM, Liu CY, Wang CH, et al. The impact of delirium on the survival of mechanically ventilated patients. Crit Care Med. 2004;32(11):2254–2259. - PubMed
-
- DeFrances CJ, Hall MJ. 2002 National Hospital Discharge Survey. Adv Data. 2004;342:1–29. - PubMed
-
- Boustani M, Buttar A. Delirium in hospitalized older adults. In: Ham R, Sloane P, Warshaw G, Bernard M, Flaherty E, editors. Primary Care Geriatrics, a Case-Based Approach. 5. Philadelphia, PA: Mosby/Elsevier; 2007. pp. 210–218.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
