

Trends in Staphylococcus aureus bacteraemia and impacts of infection control practices including universal MRSA admission screening in a hospital in Scotland, 2006-2010: retrospective cohort study and time-series intervention analysis
- PMID: 22685226
- PMCID: PMC3378947
- DOI: 10.1136/bmjopen-2011-000797
Trends in Staphylococcus aureus bacteraemia and impacts of infection control practices including universal MRSA admission screening in a hospital in Scotland, 2006-2010: retrospective cohort study and time-series intervention analysis
Abstract
Objectives: To describe secular trends in Staphylococcus aureus bacteraemia (SAB) and to assess the impacts of infection control practices, including universal methicillin-resistant Staphylococcus aureus (MRSA) admission screening on associated clinical burdens.
Design: Retrospective cohort study and multivariate time-series analysis linking microbiology, patient management and health intelligence databases.
Setting: Teaching hospital in North East Scotland.
Participants: All patients admitted to Aberdeen Royal Infirmary between 1 January 2006 and 31 December 2010: n=420 452 admissions and 1 430 052 acute occupied bed days (AOBDs).
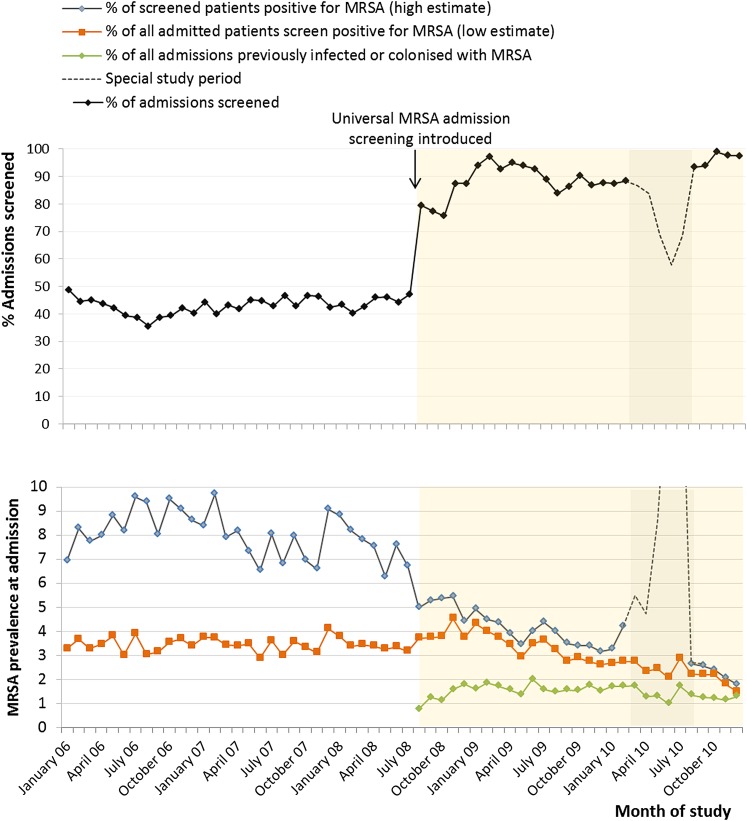
Intervention: Universal admission screening programme for MRSA (August 2008) incorporating isolation and decolonisation. PRIMARY AND SECONDARY MEASURES: Hospital-wide prevalence density, hospital-associated incidence density and death within 30 days of MRSA or methicillin-sensitive Staphylococcus aureus (MSSA) bacteraemia.
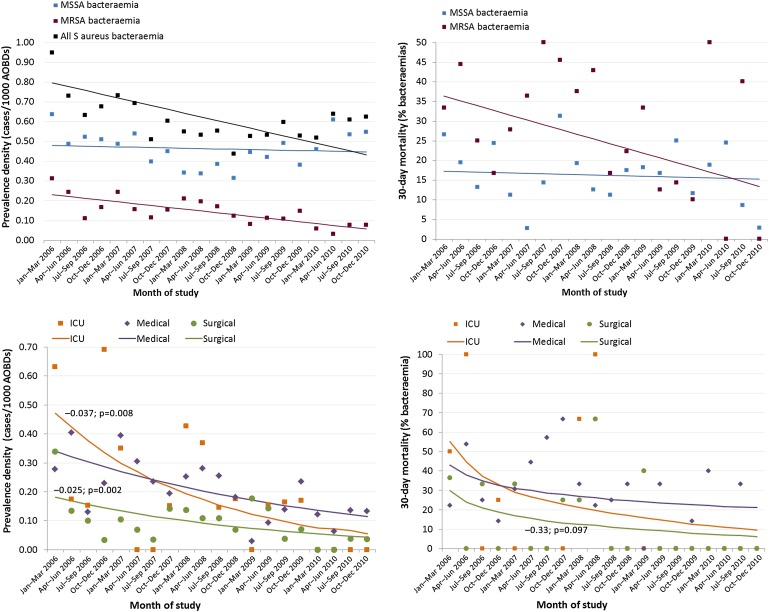
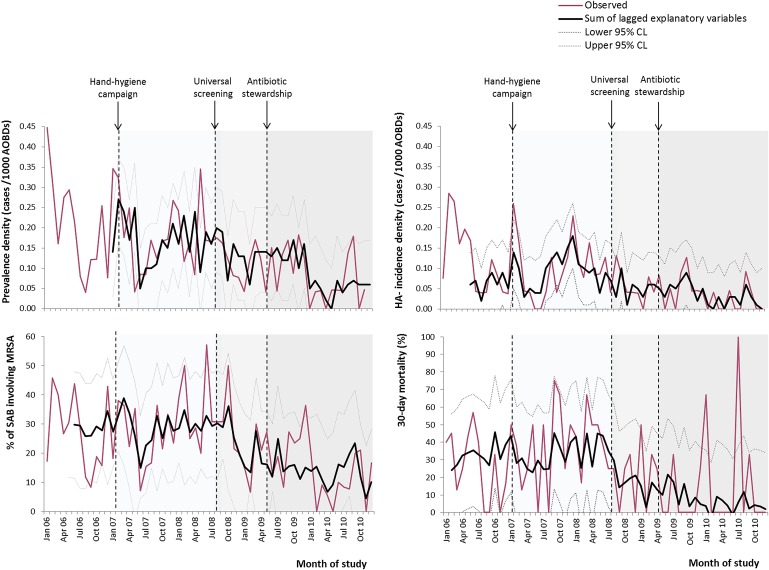
Results: Between 2006 and 2010, prevalence density of all SAB declined by 41%, from 0.73 to 0.50 cases/1000 AOBDs (p=0.002 for trend), and 30-day mortality from 26% to 14% (p=0.013). Significant reductions were observed in MRSA bacteraemia only. Overnight admissions screened for MRSA rose from 43% during selective screening to >90% within 4 months of universal screening. In multivariate time-series analysis (R(2) 0.45 to 0.68), universal screening was associated with a 19% reduction in prevalence density of MRSA bacteraemia (-0.035, 95% CI -0.049 to -0.021/1000 AOBDs; p<0.001), a 29% fall in hospital-associated incidence density (-0.029, 95% CI -0.035 to -0.023/1000 AOBDs; p<0.001) and a 46% reduction in 30-day mortality (-15.6, 95% CI -24.1% to -7.1%; p<0.001). Positive associations with fluoroquinolone and cephalosporin use suggested that antibiotic stewardship reduced prevalence density of MRSA bacteraemia by 0.027 (95% CI 0.015 to 0.039)/1000 AOBDs. Rates of MSSA bacteraemia were not significantly affected by screening or antibiotic use.
Conclusions: Declining clinical burdens from SAB were attributable to reductions in MRSA infections. Universal admission screening and antibiotic stewardship were associated with decreases in MRSA bacteraemia and associated early mortality. Control of MSSA bacteraemia remains a priority.
Conflict of interest statement
Figures

References
-
- Allegranzi B, Bagheri Nejad S, et al. Burden of endemic health-care-associated infection in developing countries: systematic review and meta-analysis. Lancet 2011;377:228–41 - PubMed
-
- Wilson J, Elgohari S, Livermore DM, et al. Trends among pathogens reported as causing bacteraemia in England, 2004-2008. Clin Microbiol Infect 2011;17:451–8 - PubMed
-
- Blot SI, Vandewoude KH, Hoste EA, et al. Outcome and attributable mortality in critically Ill patients with bacteremia involving methicillin-susceptible and methicillin-resistant Staphylococcus aureus. Arch Intern Med 2002;162:2229–35 - PubMed
LinkOut - more resources
Full Text Sources