

doi: 10.1155/2012/310206.
Epub 2012 May 21.
Update: Cytokine Dysregulation in Chronic Nonbacterial Osteomyelitis (CNO)
Affiliations
- PMID: 22685464
- PMCID: PMC3364585
- DOI: 10.1155/2012/310206
Item in Clipboard
Update: Cytokine Dysregulation in Chronic Nonbacterial Osteomyelitis (CNO)
Int J Rheumatol.
2012.
Abstract
Chronic nonbacterial osteomyelitis (CNO) with its most severe form chronic recurrent multifocal osteomyelitis (CRMO) is a non-bacterial osteitis of yet unknown origin. Secondary to the absence of both high-titer autoantibodies and autoreactive T lymphocytes, and the association with other autoimmune diseases, it was recently reclassified as an autoinflammatory disorder of the musculoskeletal system. Since its etiology is largely unknown, the diagnosis is based on clinical criteria, and treatment is empiric and not always successful. In this paper, we summarize recent advances in the understanding of possible etiopathogenetic mechanisms in CNO.
Figures
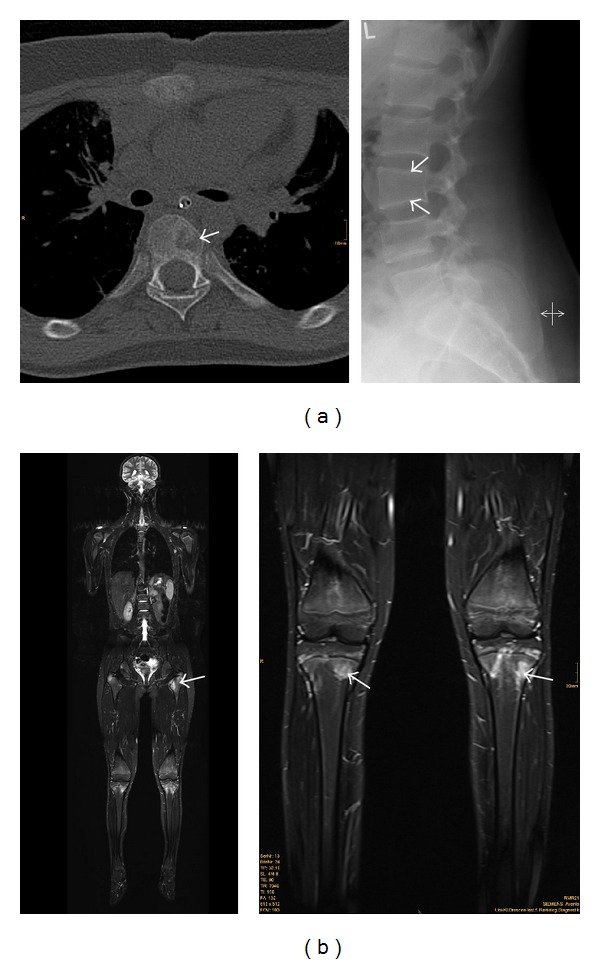
(a) left panel: computerized tomography (CT) of the spine, showing an osteolytic lesions (white arrow) in chronic recurrent multifocal osteomyelitis in a thoracic vertebra. Right panel: radiograph of the spine, showing flattening of the third lumbar vertebra (white arrows) in chronic recurrent multifocal osteomyelitis. (b) magnetic resonance imaging (MRI) in a patient with chronic recurrent multifocal osteomyelitis; left panel: whole-body MRI, showing multiple foci of osteomyelitis, some of which are distributed symmetrically; right panel: magnified image (from the left panel) of the knees, showing inflammatory epiphyseal lesions in both tibiae.
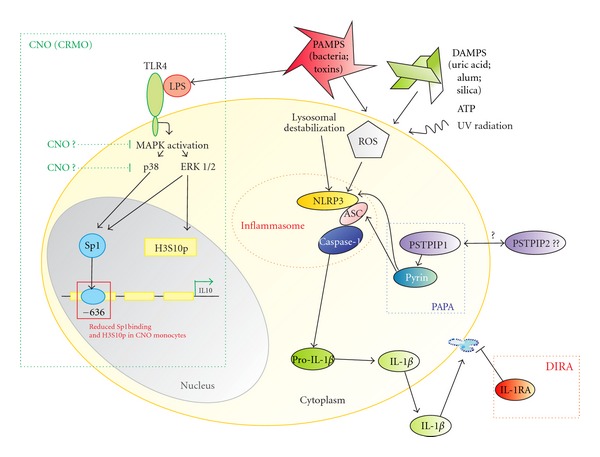
Possible pathophysiological mechanisms in autoinflammatory diseases with emphasis on CNO. Modified from [8, 9]. Endogenous and exogenous danger signals (danger-associated molecular patterns: DAMPs and pathogen-associated molecular patterns: PAMPs) activate the NLRP3 inflammasome that is involved in various autoinflammatory disorders. The exact pathways that result in NLRP3 activation are yet unknown. However, reactive oxygen species (ROS) and lysosomal destabilization seem to be involved. The selected monogenic autoinflammatory syndromes result in an activation of the caspase-1 complex. In PAPA, mutations in PSTPIP1 lead to prolonged binding of PSTPIP1 to pyrin via an SH3 domain [10] and impairment of pyrin function, resulting in constitutive activation of NLRP3, production of IL-1β, and inflammation. IL-1 receptor antagonist (IL-1RA) is a naturally occurring IL-1β antagonist, and mutations in the IL1RA gen lead to DIRA. Based on the finding that Sp1 binding to the IL10 promoter is reduced, and H3S10 phosphorylation is impaired in the same region in monocytes from CNO patients, we concluded that processes upstream of Sp1 activation and H3S10 phosphorylation may be involved. A reduced activity of MAP kinases upstream of Sp1 signalling may be responsible, resulting in reduced Sp1 activation and reduced H3S10 phosphorylation of the IL10 proximal promoter. ASC: apoptosis-associated speck-like protein containing a caspase recruitment domain; Casp1: enzymatically active caspase-1; IL-18: interleukin-18; IL-1β: interleukin-1β; NLRP3: NOD-like receptor family, pyrin domain containing 3; pro-Casp1: procaspase-1; ROS: reactive oxygen species; CNO: chronic nonbacterial osteomyelitis; DIRA: deficiency in IL-1 receptor antagonist; PAPA: pyogenic arthritis, pyoderma gangrenosum and acne; PSTPIP1: proline-serine-threonine phosphatase-interacting protein 1.
References
-
- Giedion A, Holthusen W, Masel LF, Vischer D. Subacute and chronic “symmetrical” osteomyelitis. Annales de Radiologie. 1972;15(3):329–342. - PubMed
-
- Bjorksten B, Gustavson KH, Eriksson B, Lindholm A, Nordström S. Chronic recurrent multifocal osteomyelitis and pustulosis palmoplantaris. Journal of Pediatrics. 1978;93(2):227–231. - PubMed
-
- Hamel J, Paul D, Gahr M, Hedrich CM. Pilot study: possible association of IL10 promoter polymorphisms with CRMO. Rheumatology International. 2011;32(2):555–556. - PubMed
-
- Iyer RS, Thapa MM, Chew FS. Chronic recurrent multifocal osteomyelitis: review. American Journal of Roentgenology. 2011;196(6, supplement):S87–S91. - PubMed
LinkOut - more resources
Full Text Sources
