

A comprehensive review of hypertension in pregnancy
- PMID: 22685661
- PMCID: PMC3366228
- DOI: 10.1155/2012/105918
A comprehensive review of hypertension in pregnancy
Abstract
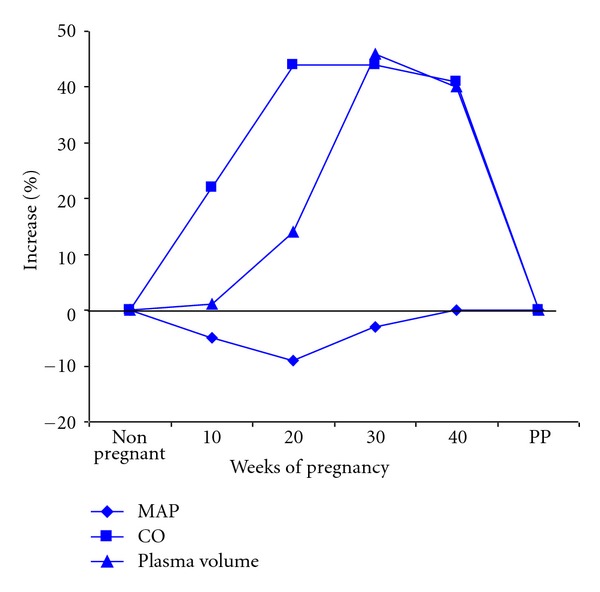
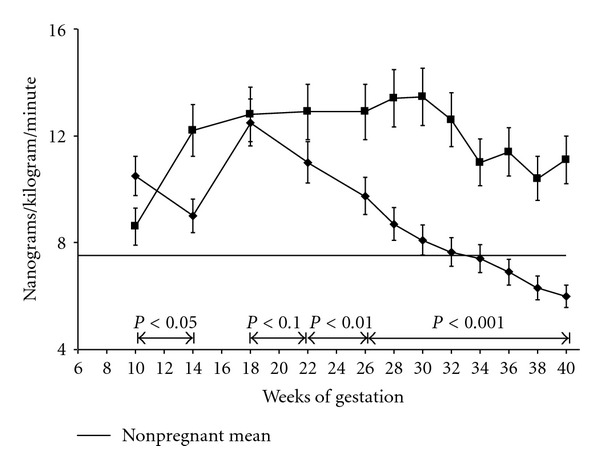
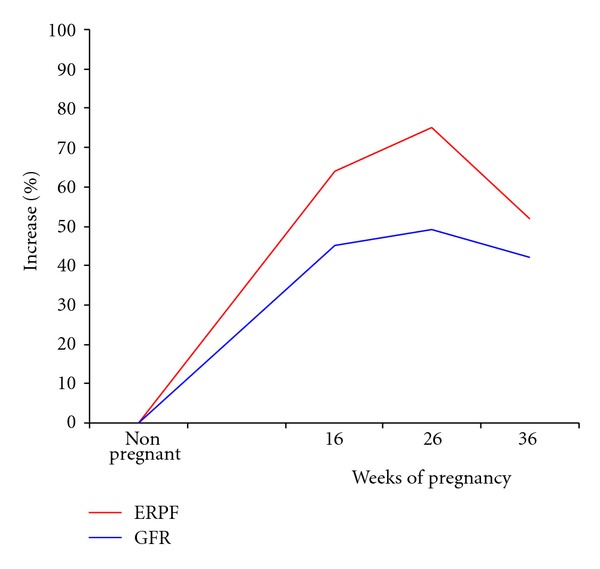
Hypertension is the most common medical disorder encountered during pregnancy. Hypertensive disorders are one of the major causes of pregnancy-related maternal deaths in the United States. We will present a comprehensive update of the literature pertinent to hypertension in pregnancy. The paper begins by defining and classifying hypertensive disorders in pregnancy. The normal vascular and renal physiological changes which occur during pregnancy are detailed. We will summarize the intriguing aspects of pathophysiology of preeclampsia, emphasizing on recent advances in this field. The existing diagnostic tools and the tests which have been proposed for screening preeclampsia are comprehensively described. We also highlight the short- and long-term implications of preeclampsia. Finally, we review the current management guidelines, goals of treatment and describe the potential risks and benefits associated with various antihypertensive drug classes. Preeclampsia still remains an enigma, and the present management focuses on monitoring and treatment of its manifestations. We are hopeful that this in depth critique will stimulate the blossoming research in the field and assist practitioners to identify women at risk and more effectively treat affected individuals.
Figures
References
-
- Roccella EJ. Report of the National High Blood Pressure Education Program Working Group on High Blood Pressure in Pregnancy. American Journal of Obstetrics & Gynecology. 2000;183(1):S1–S22. - PubMed
-
- Lindheimer MD. Introduction, history, controversies, and definitions. In: Lindheimer MD, Cunningham FG, Roberts JM, editors. Chesley's Hypertensive Disorders in Pregnancy. 3rd edition. Amsterdam, The Netherlands: Elsevier; 2009. pp. 1–24.
-
- Luft FC, Gallery EDM, Lindheimer MD. Normal and abnormal volume hemostasis. In: Lindheimer MD, Cunningham FG, Roberts JM, editors. Chesley's Hypertensive Disorders in Pregnancy. 3rd edition. Amsterdam, The Netherlands: Elsevier; 2009. pp. 271–288.
-
- Simmons LA, Gillin AG, Jeremy RW. Structural and functional changes in left ventricle during normotensive and preeclamptic pregnancy. American Journal of Physiology. 2002;283(4):H1627–H1633. - PubMed
-
- Abdul-Karim R, Assali NS. Pressor response to angiotensin in pregnant and nonpregnant women. American Journal of Obstetrics & Gynecology. 1961;82:246–251. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
