

Continuity in different care modes and its relationship to quality of life: a randomised controlled trial in patients with COPD
- PMID: 22687235
- PMCID: PMC3361122
- DOI: 10.3399/bjgp12X649115
Continuity in different care modes and its relationship to quality of life: a randomised controlled trial in patients with COPD
Abstract
Background: New care modes in primary care may affect patients' experienced continuity of care.
Aim: To analyse whether experienced continuity for patients with chronic obstructive pulmonary disease (COPD) changes after different care modes are introduced, and to analyse the relationship between continuity of care and patients' quality of life.
Design and setting: Randomised controlled trial with 2-year follow-up in general practice in the Netherlands.
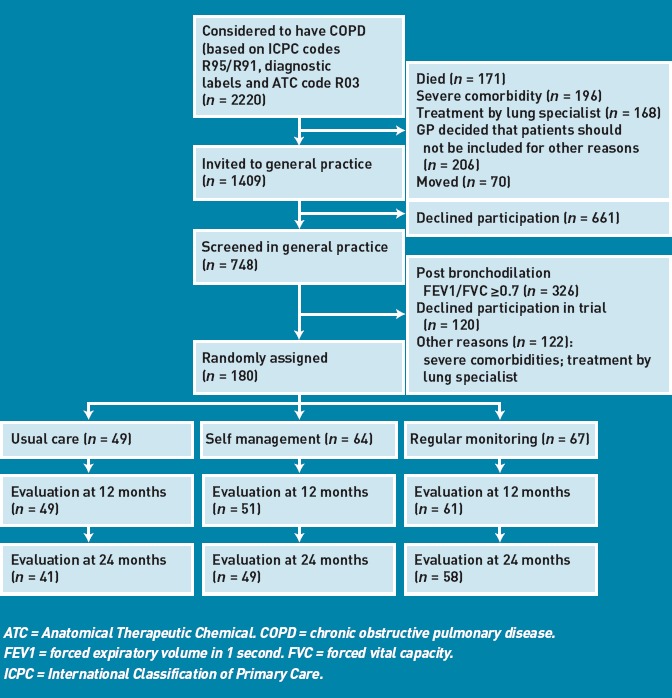
Method: A total of 180 patients with COPD were randomly assigned to three different care modes: self-management, regular monitoring by a practice nurse, and care provided by the GP at the patient's own initiative (usual care). Experienced continuity of care as personal continuity (proportion of visits with patient's own GP) and team continuity (continuity by the primary healthcare team) was measured using a self-administered patient questionnaire. Quality of life was measured using the Chronic Respiratory Questionnaire.
Results: Of the final sample (n = 148), those patients receiving usual care experienced the highest personal continuity, although the chance of not contacting any care provider was also highest in this group (29% versus 2% receiving self-management, and 5% receiving regular monitoring). There were no differences in experienced team continuity in the three care modes. No relationship was found between continuity and changes in quality of life.
Conclusion: Although personal continuity decreases when new care modes are introduced, no evidence that this affects patients' experienced team continuity or patients' quality of life was found. Patients still experienced smooth, ongoing care, and considered care to be connected. Overall, no evidence was found indicating that the introduction of new care modes in primary care for patients with COPD should be discouraged.
References
-
- Mannino DM, Buist AS. Global burden of COPD: risk factors, prevalence, and future trends. Lancet. 2007;370(9589):765–773. - PubMed
-
- Rabe KF, Beghe B, Luppi F, Fabbri LM. Update in chronic obstructive pulmonary disease 2006. Am J Respir Crit Care Med. 2007;175(12):1222–1232. - PubMed
-
- Heller KS, Solomon MZ. Continuity of care and caring: what matters to parents of children with life-threatening conditions. J Pediatr Nurs. 2005;20(5):335–346. - PubMed
-
- Schers H, van den Hoogen H, Bor H, et al. Familiarity with a GP and patients’ evaluations of care. A cross-sectional study. Fam Pract. 2005;22(1):15–19. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical