

Characterization of polymyxin B-induced nephrotoxicity: implications for dosing regimen design
- PMID: 22687519
- PMCID: PMC3421883
- DOI: 10.1128/AAC.00280-12
Characterization of polymyxin B-induced nephrotoxicity: implications for dosing regimen design
Abstract
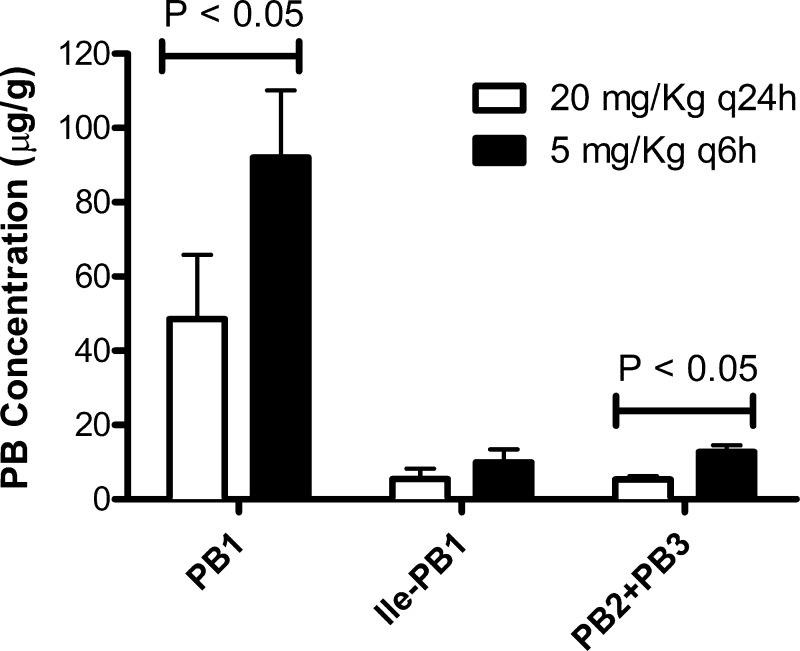
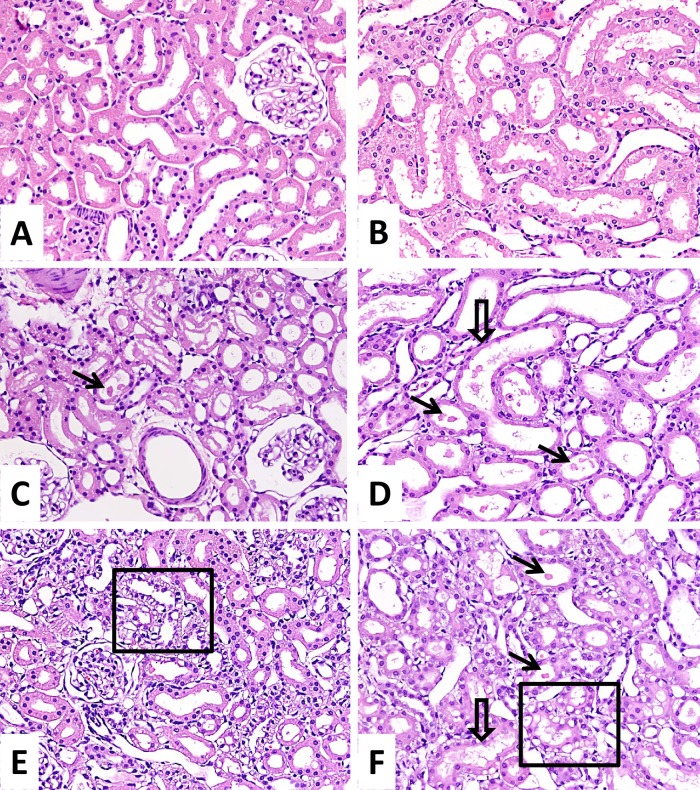
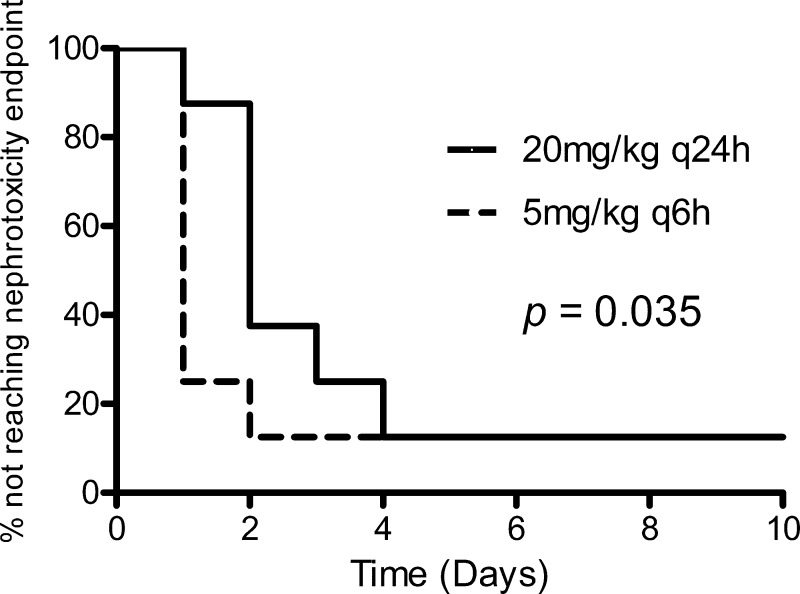
The increasing prevalence of multidrug-resistant Gram-negative infections has led to renewed interest in the use of systemic polymyxin B. However, the nephrotoxic properties of polymyxin B are still poorly understood. The objective of this study was to characterize nephrotoxicity associated with polymyxin B, with an emphasis on examining the impact of dosing frequencies on the onset of nephrotoxicity. Sprague-Dawley rats were divided into two groups and administered the same total daily dose of polymyxin B subcutaneously but with different dosing frequencies (either 20 mg/kg of body weight every 24 h [q24h] or 5 mg/kg q6h). Drug concentrations in renal tissue were compared between the two groups at 24 h. Kidney tissues were harvested at 48 h and compared histologically. Serum creatinine was measured daily for up to 10 days, and nephrotoxicity was defined as a significant elevation in serum creatinine (≥2× baseline). Kaplan-Meier analysis was used to compare the onset of nephrotoxicity. Polymyxin B-induced nephrotoxicity manifested as elevation in serum creatinine and acute tubular necrosis. Extensive injury of the proximal tubules was observed. The lesions were more severe and higher drug concentrations were achieved in the kidneys of the q6h dosing group. The q24h dosing group experienced a more gradual onset of nephrotoxicity, which could be attributed to the lower kidney tissue drug concentrations (48.5 ± 17.4 μg/g versus 92.1 ± 18.1 μg/g of polymyxin B1, P = 0.04). Preferential accumulation of polymyxin B in the kidneys suggests that uptake to renal cells is a nonpassive process and q24h dosing was less nephrotoxic than q6h dosing.
Figures
References
-
- Bhavnani SM, Rubino CM, Ambrose PG, Drusano GL. 2010. Daptomycin exposure and the probability of elevations in the creatine phosphokinase level: data from a randomized trial of patients with bacteremia and endocarditis. Clin. Infect. Dis. 50:1568–1574 - PubMed
-
- Drusano GL, et al. 2007. Back to the future: using aminoglycosides again and how to dose them optimally. Clin. Infect. Dis. 45:753–760 - PubMed
-
- Falagas ME, Rafailidis PI, Kasiakou SK, Hatzopoulou P, Michalopoulos A. 2006. Effectiveness and nephrotoxicity of colistin monotherapy vs. colistin-meropenem combination therapy for multidrug-resistant Gram-negative bacterial infections. Clin. Microbiol. Infect. 12:1227–1230 - PubMed
-
- Garnacho-Montero J, et al. 2003. Treatment of multidrug-resistant Acinetobacter baumannii ventilator-associated pneumonia (VAP) with intravenous colistin: a comparison with imipenem-susceptible VAP. Clin. Infect. Dis. 36:1111–1118 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
