

Mechanisms involved in the development and healing of diabetic foot ulceration
- PMID: 22688339
- PMCID: PMC3478547
- DOI: 10.2337/db12-0227
Mechanisms involved in the development and healing of diabetic foot ulceration
Abstract
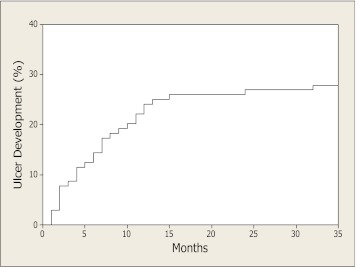
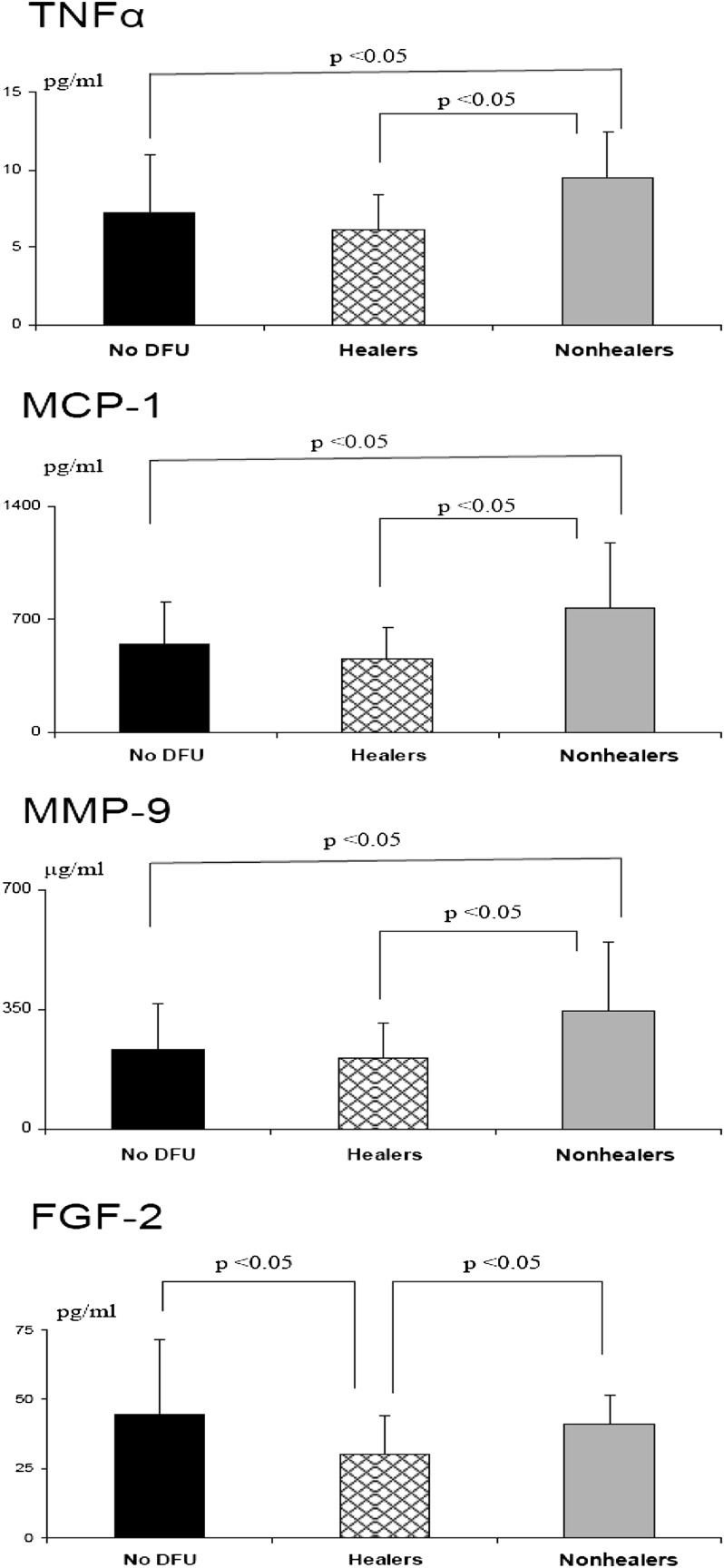
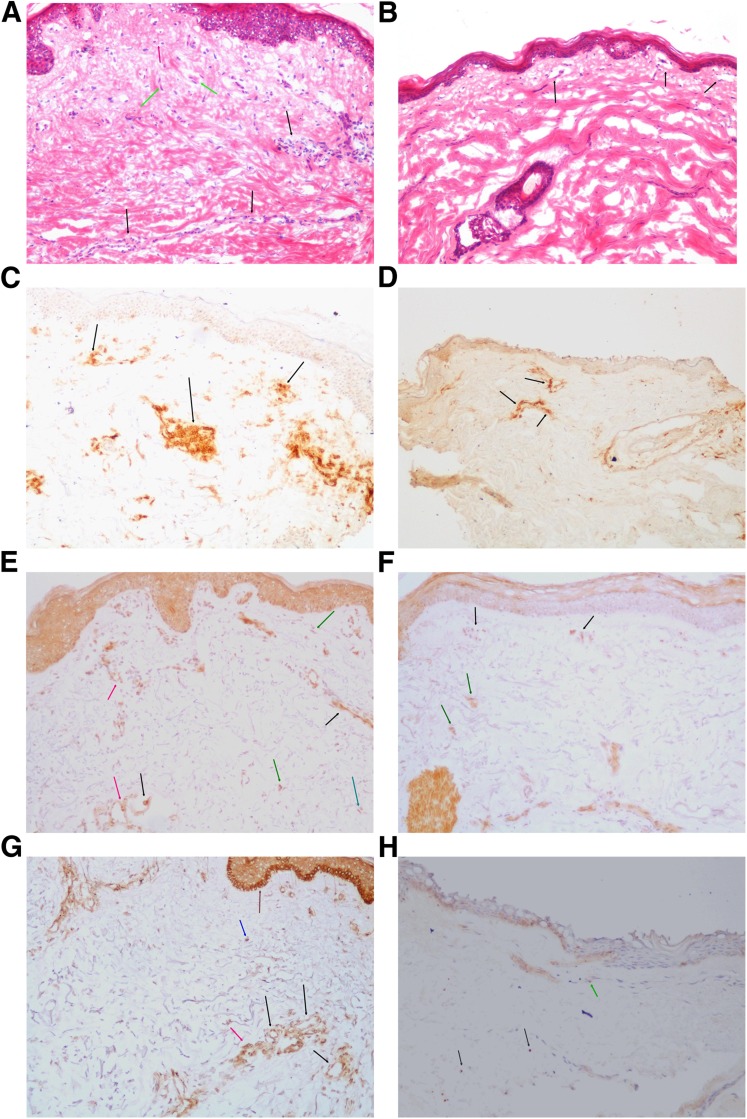
We examined the role of vascular function and inflammation in the development and failure to heal diabetic foot ulcers (DFUs). We followed 104 diabetic patients for a period of 18.4 ± 10.8 months. At the beginning of the study, we evaluated vascular reactivity and serum inflammatory cytokines and growth factors. DFUs developed in 30 (29%) patients. DFU patients had more severe neuropathy, higher white blood cell count, and lower endothelium-dependent and -independent vasodilation in the macrocirculation. Complete ulcer healing was achieved in 16 (53%) patients, whereas 13 (47%) patients did not heal. There were no differences in the above parameters between the two groups, but patients whose ulcers failed to heal had higher tumor necrosis factor-α, monocyte chemoattractant protein-1, matrix metallopeptidase 9 (MMP-9), and fibroblast growth factor 2 serum levels when compared with those who healed. Skin biopsy analysis showed that compared with control subjects, diabetic patients had increased immune cell infiltration, expression of MMP-9, and protein tyrosine phosphatase-1B (PTP1B), which negatively regulates the signaling of insulin, leptin, and growth factors. We conclude that increased inflammation, expression of MMP-9, PTP1B, and aberrant growth factor levels are the main factors associated with failure to heal DFUs. Targeting these factors may prove helpful in the management of DFUs.
Figures
References
-
- Boulton AJ, Vileikyte L, Ragnarson-Tennvall G, Apelqvist J. The global burden of diabetic foot disease. Lancet 2005;366:1719–1724 - PubMed
-
- American Diabetes Association Economic costs of diabetes in the U.S. in 2007. Diabetes Care 2008;31:596–615 - PubMed
-
- Dinh TL, Veves A. A review of the mechanisms implicated in the pathogenesis of the diabetic foot. Int J Low Extrem Wounds 2005;4:154–159 - PubMed
-
- American Diabetes Association Consensus Development Conference on Diabetic Foot Wound Care: 7–8 April 1999, Boston, Massachusetts. Diabetes Care 1999;22:1354–1360 - PubMed
-
- Pham H, Armstrong DG, Harvey C, Harkless LB, Giurini JM, Veves A. Screening techniques to identify people at high risk for diabetic foot ulceration: a prospective multicenter trial. Diabetes Care 2000;23:606–611 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
