

Case Reports
doi: 10.1136/bcr.06.2011.4296.
Right-sided diaphragmatic hernia complicated with broncho-pleuro-colonic fistula presenting as fecoptysis
Affiliations
- PMID: 22689666
- PMCID: PMC4545124
- DOI: 10.1136/bcr.06.2011.4296
Item in Clipboard
Case Reports
Right-sided diaphragmatic hernia complicated with broncho-pleuro-colonic fistula presenting as fecoptysis
BMJ Case Rep.
.
Abstract
A 37-year-old woman presented with a chief complaint of fecoptysis since 1 month. She belongs to low socio-economic status. There was no history of pulmonary tuberculosis or trauma.With the help of radiological findings, the authors were able to establish this rare diagnosis 'right-sided diaphragmatic hernia complicated with broncho-pleuro-colonic fistula presenting as fecoptysis'. Diaphragmatic hernia is a common finding in day to day practice. Fistula between bowel loops and other viscera are also common entity, but fistula between pulmonary air-way passage and colon is a rare finding. Right-sided broncho-pleuro-colonic fistula is an extremely rare entity among these conditions.
Conflict of interest statement
Figures

Plain radiograph of abdomen including chest revealed raised right dome of diaphragm with opaque right hemithorax with air-bronchogram in right mid-zone with speckled calcific foci in right side of the abdomen and chest probably suggesting faecolith.
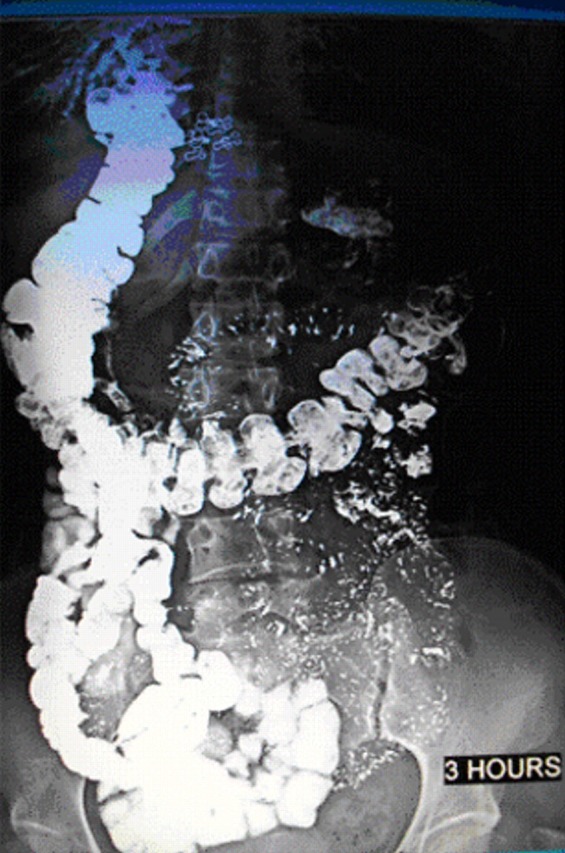
Barium meal follow through examination revealed-ascending migration of hepatic flexure and abnormal communication with pleural cavity and right lower lobe bronchus.

Plain computed axial tomography of the patient was performed and reformatted image revealed raised right dome of diaphragm with communication of hepatic flexure with right lower lobe bronchus through focal defect in right dome of diaphragm.
References
-
- Cecconi F. Arch Ital Chir (Bologna) 1958;2:84. - PubMed
-
- Keeley JL, Campbell TA. Duodenobronchofistula: with a summary of abdominothoracic fistulas. J Thoracic Cardiovasc Surg 1960;39:538. - PubMed
-
- Domej W, Kullnig P, Petritsch W, et al. Colobronchial fistula: a rare complication of Crohn’s colitis. J R Soc Med 2001;94:258–9. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical