

A case of Rosai-Dorfman disease in a pediatric patient with cardiac involvement
- PMID: 22690274
- PMCID: PMC3370701
- DOI: 10.3941/jrcr.v6i1.863
A case of Rosai-Dorfman disease in a pediatric patient with cardiac involvement
Abstract
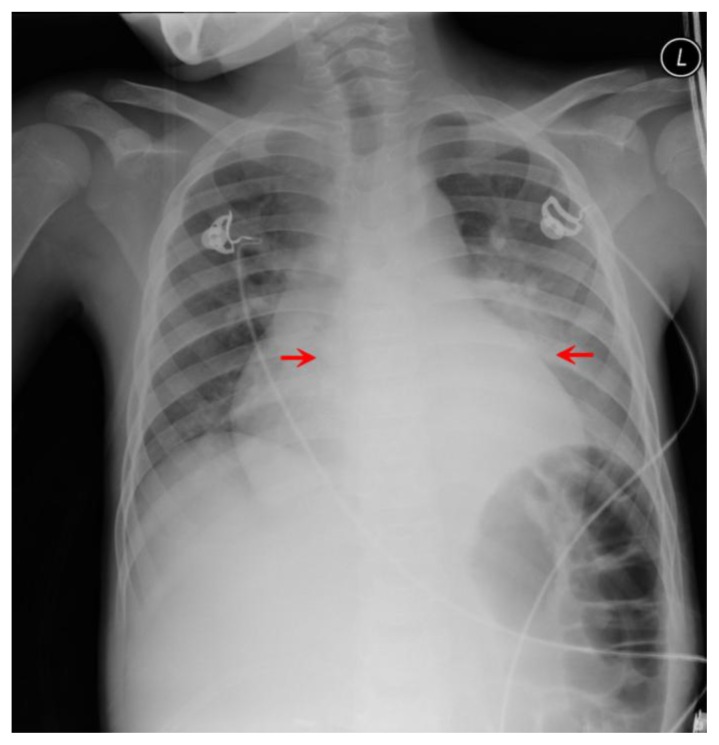
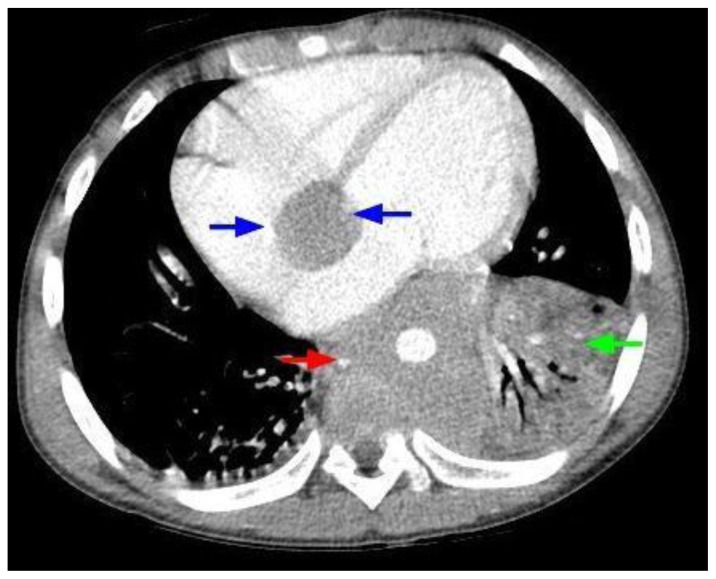
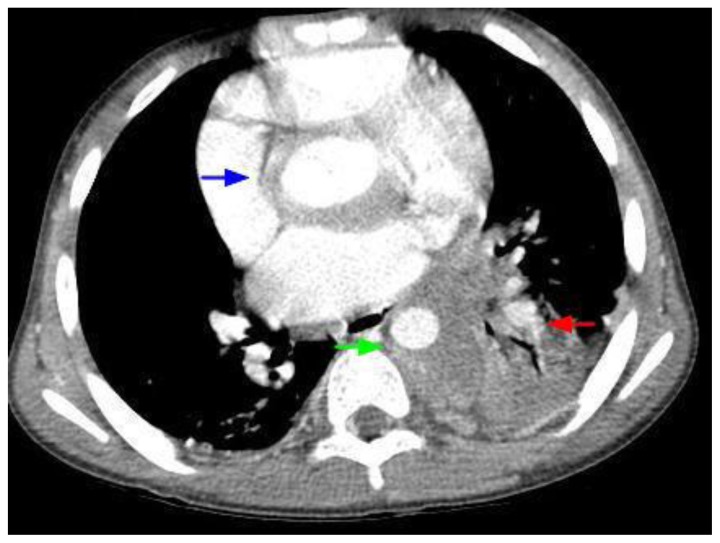
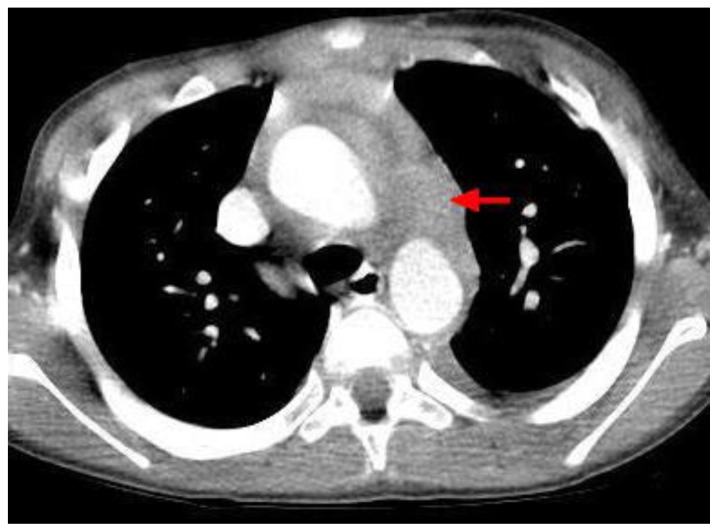
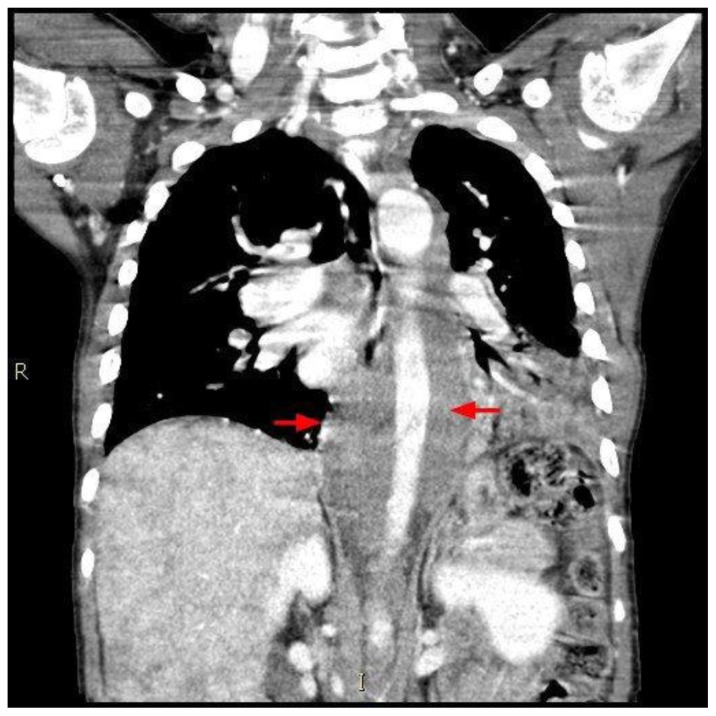
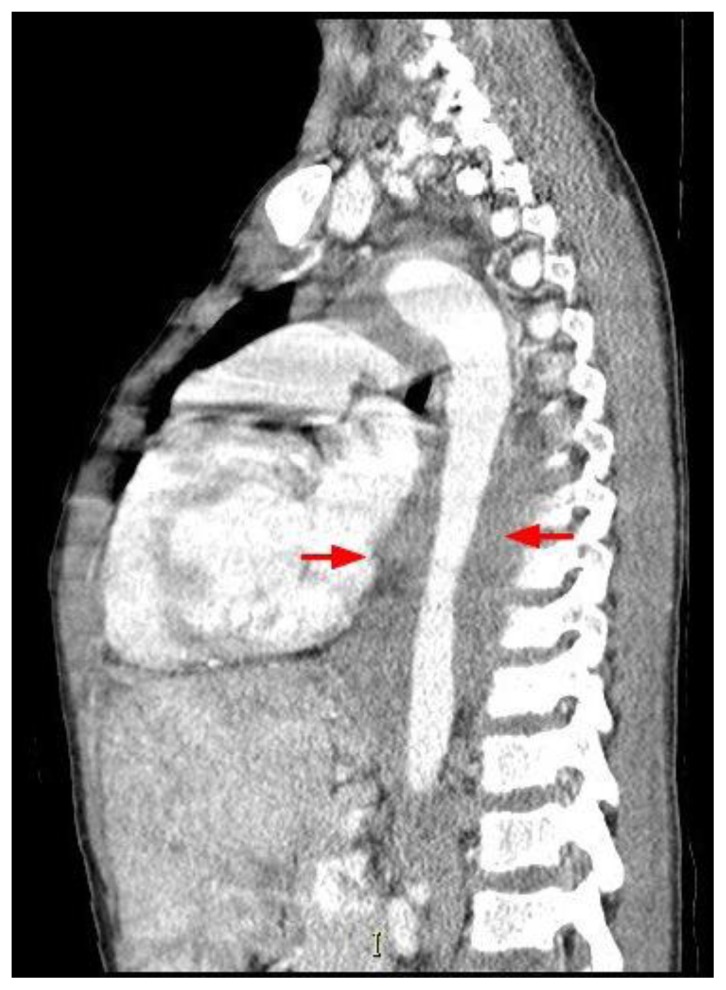
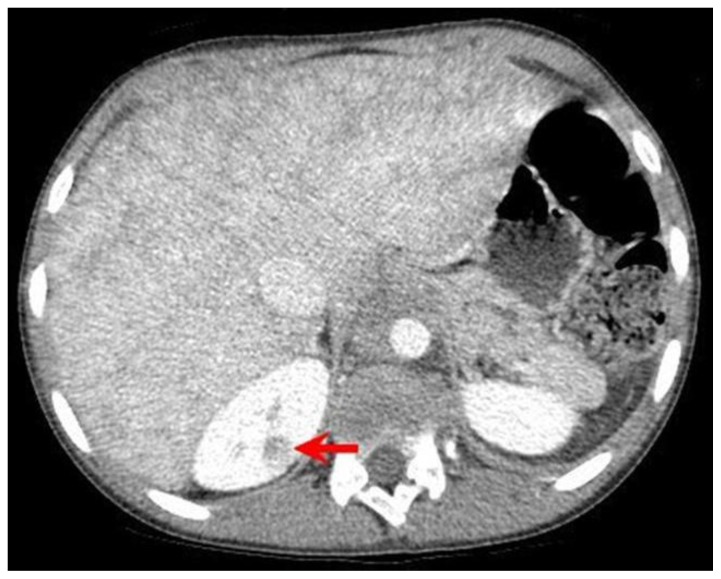
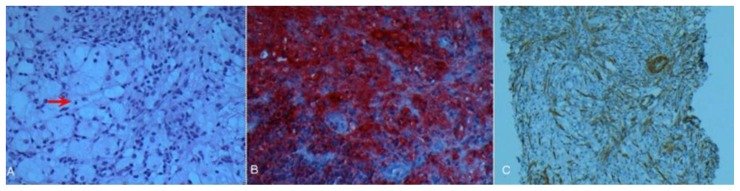
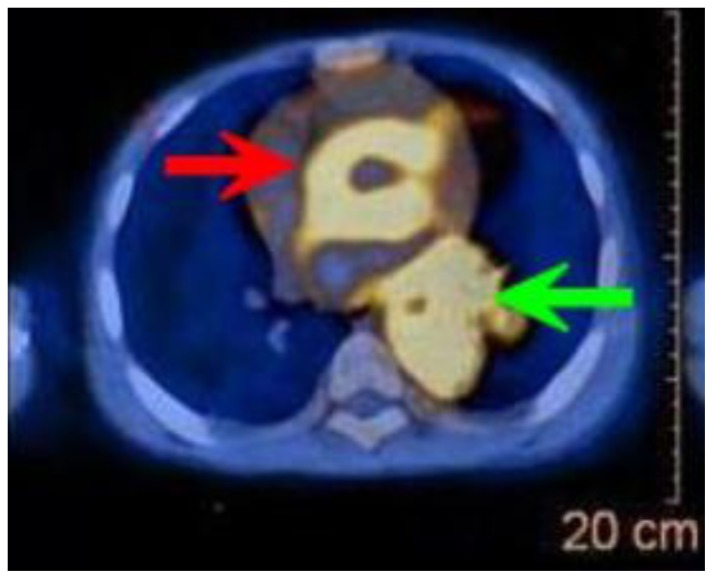
Rosai-Dorfman disease (RDD) involves abnormal proliferations of oddly behaving histocytes that are not derived from the Langerhan's Cell linage. These collections tend to occur within lymph nodes, with occasional extra nodal presentation. While RDD is a rare entity itself, extra nodal cases are even more so, with even fewer reporting cardiac involvement, and previously only in adults. This report describes the disease in a pediatric patient who had the unique feature of an extra nodal cardiac mass. The patient, who was known to have sickle cell disease, was initially erroneously thought to have acute chest syndrome. Sudden changes in the patient's status, including development of 3rd degree heart block, demanded investigation with additional imaging. Chest CT revealed a mass arising from the cardiac interatrial septum and encircling the entire thoracic aorta. Imaging features of Rosai-Dorfman disease are nonspecific, complicating the diagnosis. We present this case with discussion of this extremely uncommon entity. We describe the diagnostic methods, the differential diagnosis, and the treatment options.
Keywords: Heart; Rosai-Dorfman Disease.
Figures
References
-
- McClain K, Natkunam Y, Swerdlow S. Atypical Cellular Disorders Hematology the American Society of Hematology Education Program Book. 2004:283–96. - PubMed
-
- Rosia J, Dorfman RF. Sinus Histiocytosis with Massive Lymphadenophathy. A newly recognized benign clinicopathological entity. Archives of Pathology. 1969;87(1):63–70. - PubMed
-
- Pulsoni A, et al. Treatment of Sinus Histiocytosis with Massive Lymphadenopathy (Rosai-Dorfman Disease): Report of a case and Literature Review. American Journal of Hematology. 2002;69:67–71. - PubMed
-
- La Barge D, III, Salzman K, Harnsberger H, et al. Sinus Histiocytosis with Massive Lymphadenopathy (Rosai-Dorfman Disease): Imaging Manifestations in the Head and Neck. American Journal of Roentgenology. 2008;191:W299–306. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources