

Detection of cervical lymph node metastasis in head and neck cancer patients with clinically N0 neck-a meta-analysis comparing different imaging modalities
- PMID: 22691269
- PMCID: PMC3476985
- DOI: 10.1186/1471-2407-12-236
Detection of cervical lymph node metastasis in head and neck cancer patients with clinically N0 neck-a meta-analysis comparing different imaging modalities
Abstract
Background: How to properly manage clinically negative neck of head and neck cancer patients is a controversial topic. Research is now directed toward finding a method sensitive enough to bring the risk of occult metastases below 20%. The aim of this review was to compare the diagnostic accuracy of different imaging modalities, including CT, MRI, PET and US, in clinically N0 head and neck cancer patients.
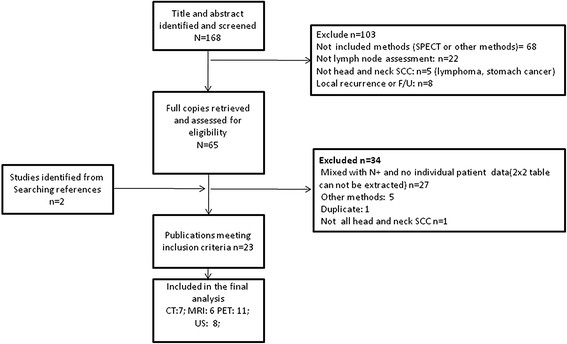
Methods: For this systematic review and meta-analysis, PubMed and the Cochrane Database were searched for relevant original articles published up to May 2011. Inclusion criteria were as follows: articles were reported in English; CT, MRI, PET or US were performed to identify cervical metastases in clinically N0 head and neck squamous cell carcinoma; and data were sufficient for the calculation of true-positive or false-negative values. A bivariate random effect model was used to obtain pooled sensitivity and specificity. The positive and negative test probability of neck metastasis was generated based on Bayesian theory and collected data for different pre-test possibilities.
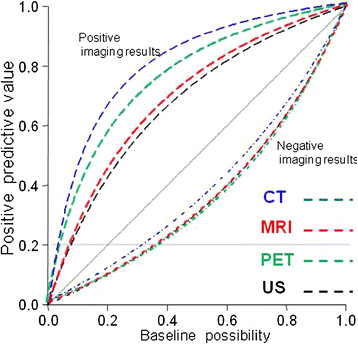
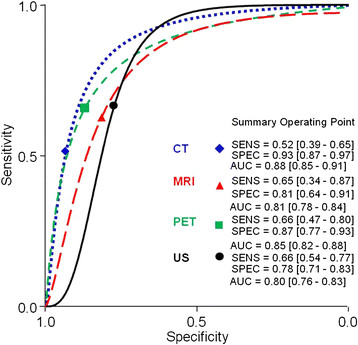
Results: Of the 168 identified relevant articles, 7 studies fulfilled all inclusion criteria for CT, 6 studies for MRI, 11 studies for PET and 8 studies for US. There was no difference in sensitivity and specificity among these imaging modalities, except CT was superior to US in specificity. The pooled estimates for sensitivity were 52% (95% confidence interval [CI], 39% ~ 65%), 65% (34 ~ 87%) 66% (47 ~ 80%), and 66% (45 ~ 77%), on a per-neck basis for CT, MRI, PET and US, respectively. The pooled estimates for specificity were 93% (87% ~ 97%), 81% (64 ~ 91%), 87% (77 ~ 93%), and 78% (71 ~ 83%) for CT, MRI, PET and US, respectively. With pre-examination nodal metastasis probabilities set at 10%, 20% and 30%, the post-exam probabilities of positive nodal metastasis rates were 47%, 66% and 77% for CT; 27%, 46% and 59% for MRI; 36%, 56% and 69% for PET; and 25%, 42% and 56% for US, respectively. Negative nodal metastasis probabilities were 95%, 89% and 82% for CT; 95%, 90% and 84% for MRI; 96%, 91% and 86% for PET; and 95%, 90% and 84% for US, respectively.
Conclusions: Modern imaging modalities offer similar diagnostic accuracy to define and diagnose clinically N0 neck. Minimizing morbidity and avoiding elective neck dissection is acceptable in some select cases.
Figures
References
-
- van den Brekel MW, Castelijns JA, Stel HV, Golding RP, Meyer CJ, Snow GB. Modern imaging techniques and ultrasound-guided aspiration cytology for the assessment of neck node metastases: a prospective comparative study. Eur Arch Otorhinolaryngol. 1993;250:11–17. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
