

Clinical target volume delineation including elective nodal irradiation in preoperative and definitive radiotherapy of pancreatic cancer
- PMID: 22691275
- PMCID: PMC3494529
- DOI: 10.1186/1748-717X-7-86
Clinical target volume delineation including elective nodal irradiation in preoperative and definitive radiotherapy of pancreatic cancer
Abstract
Background: Radiotherapy (RT) is widely used in the treatment of pancreatic cancer. Currently, recommendation has been given for the delineation of the clinical target volume (CTV) in adjuvant RT. Based on recently reviewed pathologic data, the aim of this study is to propose criteria for the CTV definition and delineation including elective nodal irradiation (ENI) in the preoperative and definitive treatment of pancreatic cancer.
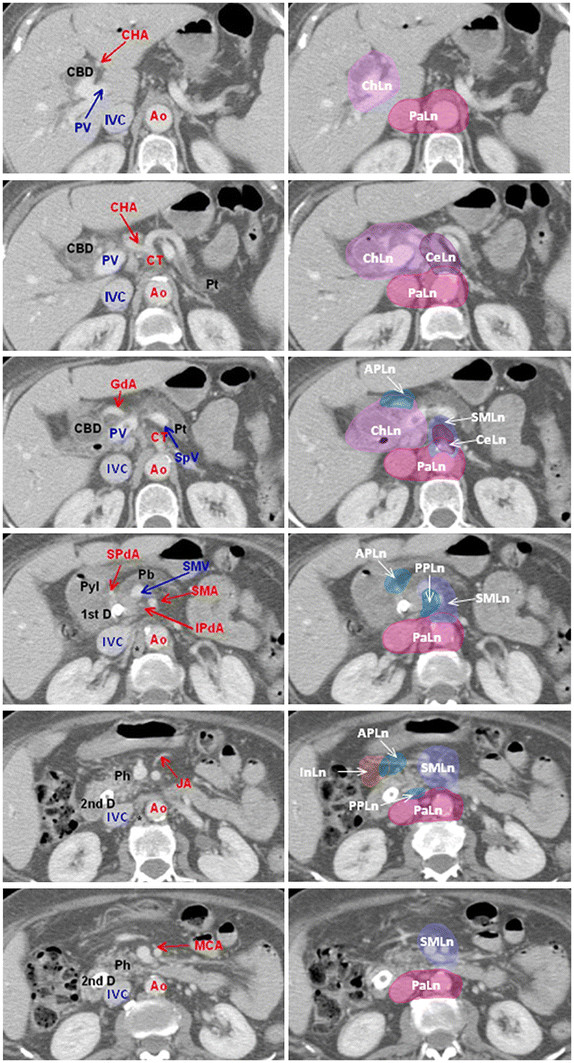
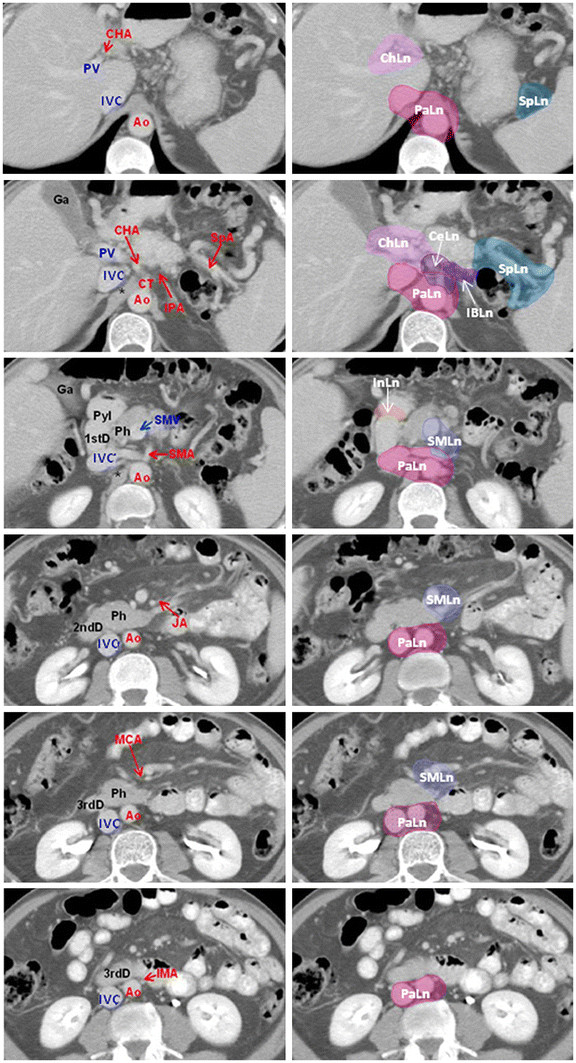
Methods: The anatomical structures of interest, as well as the abdominal vasculature were identified on intravenous contrast-enhanced CT scans of two different patients with pancreatic cancer of the head and the body. To delineate the lymph node area, a margin of 10 mm was added to the arteries.
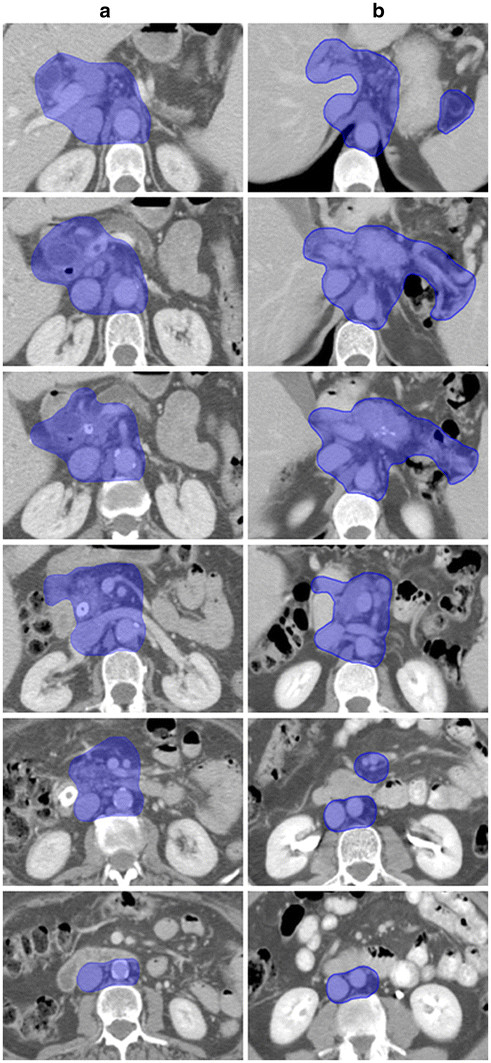
Results: We proposed a set of guidelines for elective treatment of high-risk nodal areas and CTV delineation. Reference CT images were provided.
Conclusions: The proposed guidelines could be used for preoperative or definitive RT for carcinoma of the head and body of the pancreas. Further clinical investigations are needed to validate the defined CTVs.
Figures
Similar articles
-
Radiation Therapy Oncology Group consensus panel guidelines for the delineation of the clinical target volume in the postoperative treatment of pancreatic head cancer.Int J Radiat Oncol Biol Phys. 2012 Jul 1;83(3):901-8. doi: 10.1016/j.ijrobp.2012.01.022. Epub 2012 Apr 5. Int J Radiat Oncol Biol Phys. 2012. PMID: 22483737 Free PMC article. Clinical Trial.
-
Inter-observer variability of clinical target volume delineation in radiotherapy treatment of pancreatic cancer: a multi-institutional contouring experience.Radiat Oncol. 2014 Sep 8;9:198. doi: 10.1186/1748-717X-9-198. Radiat Oncol. 2014. PMID: 25199768 Free PMC article.
-
Proposing the lymphatic target volume for elective radiation therapy for pancreatic cancer: a pooled analysis of clinical evidence.Radiat Oncol. 2010 Apr 15;5:28. doi: 10.1186/1748-717X-5-28. Radiat Oncol. 2010. PMID: 20398316 Free PMC article.
-
Elective clinical target volumes for conformal therapy in anorectal cancer: a radiation therapy oncology group consensus panel contouring atlas.Int J Radiat Oncol Biol Phys. 2009 Jul 1;74(3):824-30. doi: 10.1016/j.ijrobp.2008.08.070. Epub 2008 Dec 29. Int J Radiat Oncol Biol Phys. 2009. PMID: 19117696 Free PMC article.
-
NRG Oncology International Consensus Contouring Atlas on Target Volumes and Dosing Strategies for Dose-Escalated Pancreatic Cancer Radiation Therapy.Int J Radiat Oncol Biol Phys. 2025 Mar 15;121(4):918-929. doi: 10.1016/j.ijrobp.2024.10.026. Epub 2024 Nov 6. Int J Radiat Oncol Biol Phys. 2025. PMID: 39510320 Review.
Cited by
-
Para-aortic lymph node metastasis in lower Thoracic Esophageal Squamous Cell Carcinoma after Radical Esophagectomy: a CT-based atlas and its clinical implications for Adjuvant Radiotherapy.J Cancer. 2021 Jan 18;12(6):1734-1741. doi: 10.7150/jca.51212. eCollection 2021. J Cancer. 2021. PMID: 33613762 Free PMC article.
-
Post-radiation neutrophil-to-lymphocyte ratio is a prognostic marker in patients with localized pancreatic adenocarcinoma treated with anti-PD-1 antibody and stereotactic body radiation therapy.Radiat Oncol J. 2022 Jun;40(2):111-119. doi: 10.3857/roj.2021.01060. Epub 2022 May 20. Radiat Oncol J. 2022. PMID: 35796114 Free PMC article.
-
An atlas for clinical target volume definition, including elective nodal irradiation in definitive radiotherapy of biliary cancer.Oncol Lett. 2019 Feb;17(2):1784-1790. doi: 10.3892/ol.2018.9774. Epub 2018 Nov 28. Oncol Lett. 2019. PMID: 30675238 Free PMC article.
-
Successful radiation treatment of chylous ascites following pancreaticoduodenectomy.Strahlenther Onkol. 2015 May;191(5):448-52. doi: 10.1007/s00066-014-0805-z. Epub 2015 Jan 10. Strahlenther Onkol. 2015. PMID: 25575979
-
Patterns of Recurrence After Primary Local Therapy for Pancreatic Ductal Adenocarcinoma - A Critical Review of Rationale and Target Delineation for (Neo)Adjuvant Radiation Therapy.Pract Radiat Oncol. 2022 Nov-Dec;12(6):e463-e473. doi: 10.1016/j.prro.2022.06.004. Epub 2022 Jun 17. Pract Radiat Oncol. 2022. PMID: 35718073 Free PMC article. Review.
References
-
- Gastrointestinal Tumor Study Group. Further evidence of effective adjuvant combined radiation and chemotherapy following curative resection of pancreatic cancer. Cancer. 1987;59:2006–2010. - PubMed
-
- Klinkenbijl JH, Jeekel J, Sahmoud T, van Pel R, Couvreur ML, Veenhof CH, Arnaud JP, Gonzalez DG, de Wit LT, Hennipman A, Wils J. Adjuvant radiotherapy and 5-fluorouracil after curative resection for the cancer of the pancreas and periampullary region: phase III trial of the EORTC Gastrointestinal Tract Cancer Cooperative Group. Ann Surg. 1999;230:776–784. doi: 10.1097/00000658-199912000-00006. - DOI - PMC - PubMed
-
- Khanna A, Walker GR, Livingstone AS, Arheart KL, Rocha-Lima C, Koniaris LG. Is adjuvant 5-FU based chemoradiotherapy for resectable pancreatic adenocarcinoma beneficial? A meta-analysis of an unanswered question. J Gastrointest Surg. 2006;10:689–697. doi: 10.1016/j.gassur.2005.11.006. - DOI - PubMed
-
- Stocken DD, Büchler MW, Dervenis C, Bassi C, Jeekel H, Klinkenbijl JH, Bakkevold KE, Takada T, Amano H, Neoptolemos JP. Pancreatic Cancer Meta-analysis Group. Meta-analysis of randomised adjuvant therapy trials for pancreatic cancer. Br J Cancer. 2005;92:1372–1381. doi: 10.1038/sj.bjc.6602513. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
