

Achieving routine submillisievert CT scanning: report from the summit on management of radiation dose in CT
- PMID: 22692035
- PMCID: PMC3401354
- DOI: 10.1148/radiol.12112265
Achieving routine submillisievert CT scanning: report from the summit on management of radiation dose in CT
Abstract
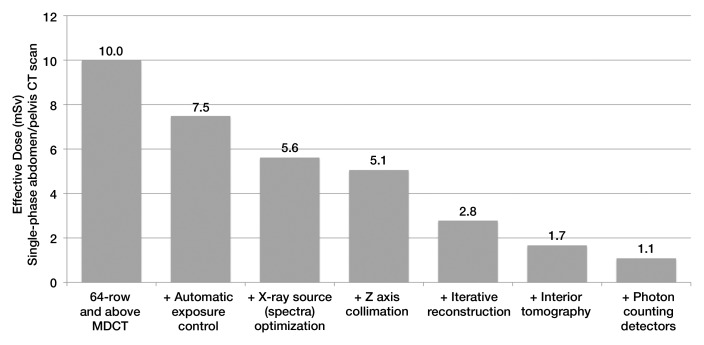
This Special Report presents the consensus of the Summit on Management of Radiation Dose in Computed Tomography (CT) (held in February 2011), which brought together participants from academia, clinical practice, industry, and regulatory and funding agencies to identify the steps required to reduce the effective dose from routine CT examinations to less than 1 mSv. The most promising technologies and methods discussed at the summit include innovations and developments in x-ray sources; detectors; and image reconstruction, noise reduction, and postprocessing algorithms. Access to raw projection data and standard data sets for algorithm validation and optimization is a clear need, as is the need for new, clinically relevant metrics of image quality and diagnostic performance. Current commercially available techniques such as automatic exposure control, optimization of tube potential, beam-shaping filters, and dynamic z-axis collimators are important, and education to successfully implement these methods routinely is critically needed. Other methods that are just becoming widely available, such as iterative reconstruction, noise reduction, and postprocessing algorithms, will also have an important role. Together, these existing techniques can reduce dose by a factor of two to four. Technical advances that show considerable promise for additional dose reduction but are several years or more from commercial availability include compressed sensing, volume of interest and interior tomography techniques, and photon-counting detectors. This report offers a strategic roadmap for the CT user and research and manufacturer communities toward routinely achieving effective doses of less than 1 mSv, which is well below the average annual dose from naturally occurring sources of radiation.
Figures
Comment in
-
Radiation exposure in CT scanning and risk: where are we?Radiology. 2012 Aug;264(2):325-8. doi: 10.1148/radiol.12121137. Radiology. 2012. PMID: 22821692 No abstract available.
References
-
- International Commission on Radiological Protection Recommendations of the International Commission on Radiological Protection (ICRP report no. 26). Oxford, England: International Commission on Radiological Protection, 1977
-
- McCollough CH, Schueler BA. Calculation of effective dose. Med Phys 2000;27(5):828–837 - PubMed
-
- 1990 Recommendations of the International Commission on Radiological Protection. Ann ICRP 1991;21(1-3):1–201 - PubMed
-
- The 2007 Recommendations of the International Commission on Radiological Protection ICRP publication 103. Ann ICRP 2007;37(2-4):1–332 - PubMed
-
- Menzel HG, Clement C, DeLuca P. ICRP publication 110. Realistic reference phantoms: an ICRP/ICRU joint effort. A report of adult reference computational phantoms. Ann ICRP 2009;39(2):1–164 [Published correction appears in Ann ICRP 2009;39(2):165.] - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
