

Impact of sarcopenia on outcomes following resection of pancreatic adenocarcinoma
- PMID: 22692586
- PMCID: PMC3578313
- DOI: 10.1007/s11605-012-1923-5
Impact of sarcopenia on outcomes following resection of pancreatic adenocarcinoma
Abstract
Introduction: Assessing patient-specific risk factors for long-term mortality following resection of pancreatic adenocarcinoma can be difficult. Sarcopenia--the measurement of muscle wasting--may be a more objective and comprehensive patient-specific factor associated with long-term survival.
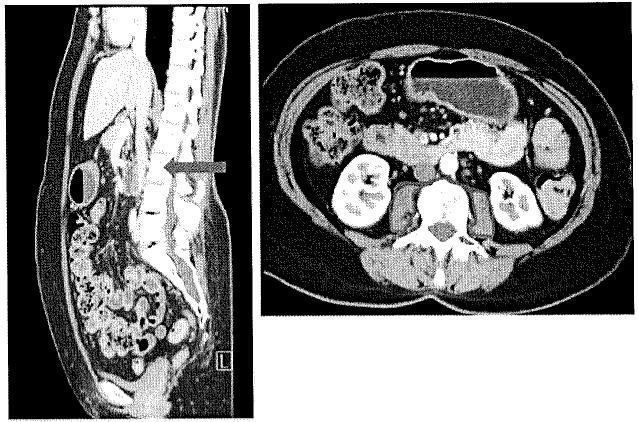
Methods: Total psoas area (TPA) was measured on preoperative cross-sectional imaging in 557 patients undergoing resection of pancreatic adenocarcinoma between 1996 and 2010. Sarcopenia was defined as the presence of a TPA in the lowest sex-specific quartile. The impact of sarcopenia on 90-day, 1-year, and 3-year mortality was assessed relative to other clinicopathological factors.
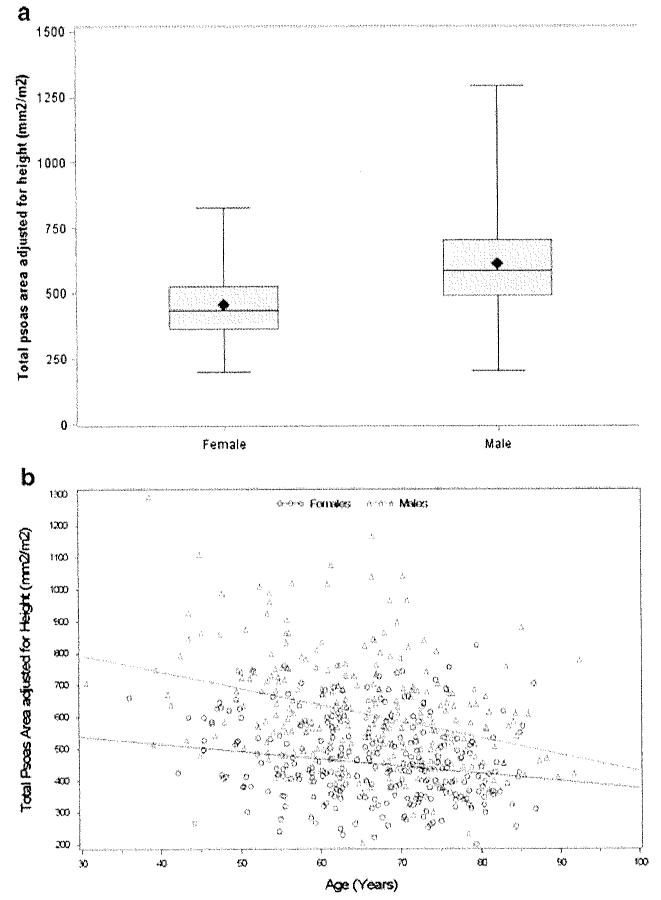
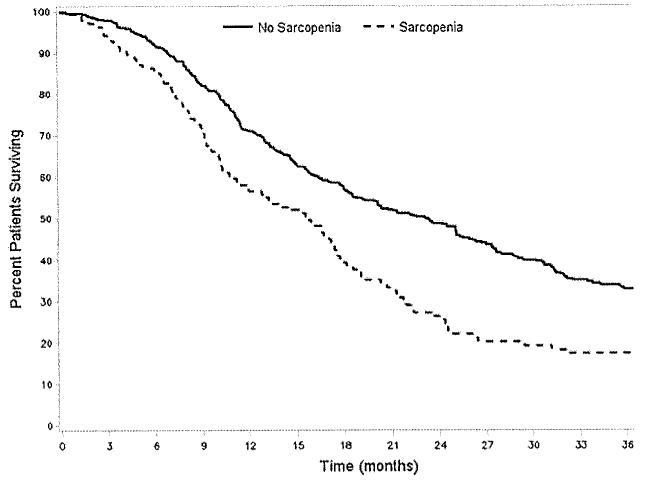
Results: Mean patient age was 65.7 years and 53.1 % was male. Mean TPA among men (611 mm²/m²) was greater than among women (454 mm²/m²). Surgery involved pancreaticoduodenectomy (86.0 %) or distal pancreatectomy (14.0 %). Mean tumor size was 3.4 cm; 49.9 % and 88.5 % of patients had vascular and perineural invasion, respectively. Margin status was R0 (59.0 %) and 77.7 % patients had lymph node metastasis. Overall 90-day mortality was 3.1 % and overall 1- and 3-year survival was 67.9 % and 35.7 %, respectively. Sarcopenia was associated with increased risk of 3-year mortality (HR = 1.68; P < 0.001). Tumor-specific factors such as poor differentiation on histology (HR = 1.75), margin status (HR = 1.66), and lymph node metastasis (HR = 2.06) were associated with risk of death at 3-years (all P < 0.001). After controlling for these factors, sarcopenia remained independently associated with an increased risk of death at 3 years (HR = 1.63; P < 0.001).
Conclusions: Sarcopenia was a predictor of survival following pancreatic surgery, with sarcopenic patients having a 63 % increased risk of death at 3 years. Sarcopenia was an objective measure of patient frailty that was strongly associated with long-term outcome independent of tumor-specific factors.
Figures
References
-
- Sohn TA, Yeo CJ, Cameron JL, et al. Resected adenocarcinoma of the pancreas-616 patients: results, outcomes, and prognostic indicators. J Gastrointest Surg. 2000;4(6):567–79. - PubMed
-
- Oettle H, Post S, Neuhaus P, et al. Adjuvant chemotherapy with gemcitabine vs observation in patients undergoing curative-intent resection of pancreatic cancer: a randomized controlled trial. JAMA. 2007;297(3):267–77. - PubMed
-
- Klinkenbijl JH, Jeekel J, Sahmoud T, et al. Adjuvant radiotherapy and 5-fluorouracil after curative resection of cancer of the pancreas and periampullary region: phase III trial of the EORTC gastrointestinal tact cancer cooperative group. Ann Surg. 1999;230(6):776–82. discussion 82-4. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
