

AMG 386 in combination with sorafenib in patients with metastatic clear cell carcinoma of the kidney: a randomized, double-blind, placebo-controlled, phase 2 study
- PMID: 22692704
- PMCID: PMC4666535
- DOI: 10.1002/cncr.27632
AMG 386 in combination with sorafenib in patients with metastatic clear cell carcinoma of the kidney: a randomized, double-blind, placebo-controlled, phase 2 study
Abstract
Background: This study evaluated the tolerability and antitumor activity of AMG 386, a peptibody (a peptide Fc fusion) that neutralizes the interaction of angiopoietin-1 and angiopoietin-2 with Tie2 (tyrosine kinase with immunoglobulin-like and EGF-like domains 2), plus sorafenib in patients with clear cell metastatic renal cell carcinoma (mRCC) in a randomized controlled study.
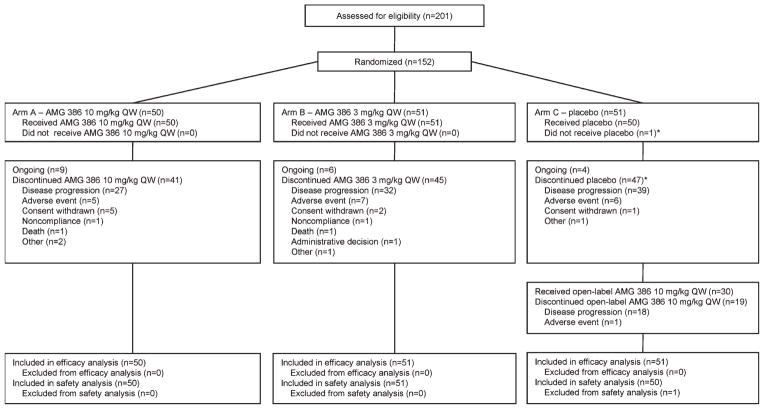
Methods: Previously untreated patients with mRCC were randomized 1:1:1 to receive sorafenib 400 mg orally twice daily plus intravenous AMG 386 at 10 mg/kg (arm A) or 3 mg/kg (arm B) or placebo (arm C) once weekly (qw). Patients in arm C could receive open-label AMG 386 at 10 mg/kg qw plus sorafenib following disease progression. The primary endpoint was progression-free survival (PFS).
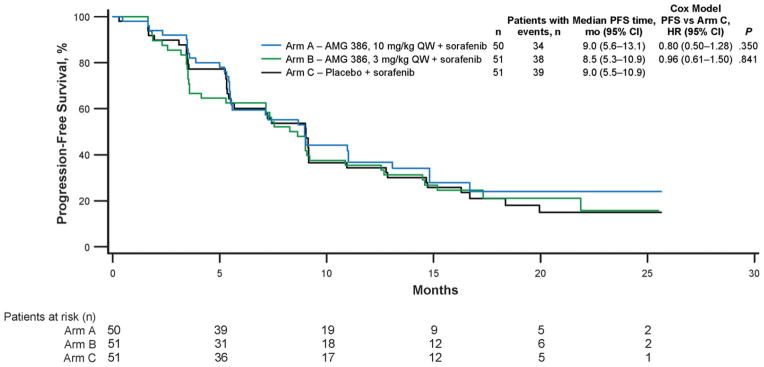
Results: A total of 152 patients were randomized. Median PFS was 9.0, 8.5, and 9.0 months in arms A, B, and C, respectively (hazard ratio for arms A and B vs arm C, 0.88; 95% confidence interval [CI], 0.60-1.30; P = .523). The objective response rate (95% CI) for arms A, B, and C, respectively, was 38% (25%-53%), 37% (24%-52%), and 25% (14%-40%). Among 30 patients in arm C who had disease progression and subsequently received open-label AMG 386 at 10 mg/kg qw, the objective response rate was 3% (95% CI, 0%-17%). Frequently occurring adverse events (AEs) included diarrhea (arms A/B/C, 70%/67%/56%), palmar-plantar erythrodysesthesia syndrome (52%/47%/54%), alopecia (50%/45%/50%), and hypertension (42%/49%/46%). Fifteen patients had grade 4 AEs (arms A/B/C, n = 3/7/5); 4 had fatal AEs (n = 2/1/1), with 1 (abdominal pain, arm B) considered possibly related to AMG 386.
Conclusions: In patients with mRCC, AMG 386 plus sorafenib was tolerable but did not significantly improve PFS compared with placebo plus sorafenib.
Trial registration: ClinicalTrials.gov NCT00467025.
Copyright © 2012 American Cancer Society.
Conflict of interest statement
CONFLICT OF INTEREST DISCLOSURE
Dr. Rini has been a consultant for and has received research funding from Amgen. Dr. Tannir has been a consultant and has received honoraria from Pfizer, Abbott, and Novartis, and has received research funding from Abbott, Amgen, and Pfizer. Dr. Fishman has been a consultant for Aveo, Eisai, GlaxoSmithKline, Genentech, Seattle Genetics, Pfizer, Novartis, Prometheus, and Altor, has received honoraria from Aveo, Bayer, Pfizer, Novartis, Genentech, Eisai, and GlaxoSmithKline, and research funding from Amgen, Altor, Aveo, FDA, NCI, Southwest Oncology Group, Bayer, Pfizer, Genentech, and Eli Lilly. Dr. Escudier has been a consultant for Bayer, Pfizer, and Roche, and has received honoraria from Bayer, Roche, Pfizer, Genentech, Novartis, and Aveo. Ms. Kracht and Drs. Sun, Bass, and Puhlmann are Amgen employees/shareholders. Dr. Ravaud has been a consultant for Pfizer, Novartis, Bayer, GlaxoSmithKline, Dendreon, and Aveo, has received travel expenses from Novartis and Pfizer, and research funding from Pfizer and Roche. All other authors made no disclosures.
Figures
References
-
- Rini BI, Campbell SC, Escudier B. Renal cell carcinoma. Lancet. 2009;373:1119–1132. - PubMed
-
- Rini BI. New strategies in kidney cancer: therapeutic advances through understanding the molecular basis of response and resistance. Clin Cancer Res. 2010;16:1348–1354. - PubMed
-
- Currie MJ, Gunningham SP, Turner K, et al. Expression of the angiopoietins and their receptor Tie2 in human renal clear cell carcinomas; regulation by the von Hippel-Lindau gene and hypoxia. J Pathol. 2002;198:502–510. - PubMed
-
- Bullock AJ, Zhang A, O’Neill A, et al. Plasma angiopoietin-2 (ANG2) as an angiogenic biomarker in renal cell carcinoma (RCC) [Abstract] J Clin Oncol. 2010;28:4630.
Publication types
MeSH terms
Substances
Supplementary concepts
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
