

Maximum Recommended Dosage of Lithium for Pregnant Women Based on a PBPK Model for Lithium Absorption
- PMID: 22693500
- PMCID: PMC3369391
- DOI: 10.1155/2012/352729
Maximum Recommended Dosage of Lithium for Pregnant Women Based on a PBPK Model for Lithium Absorption
Abstract
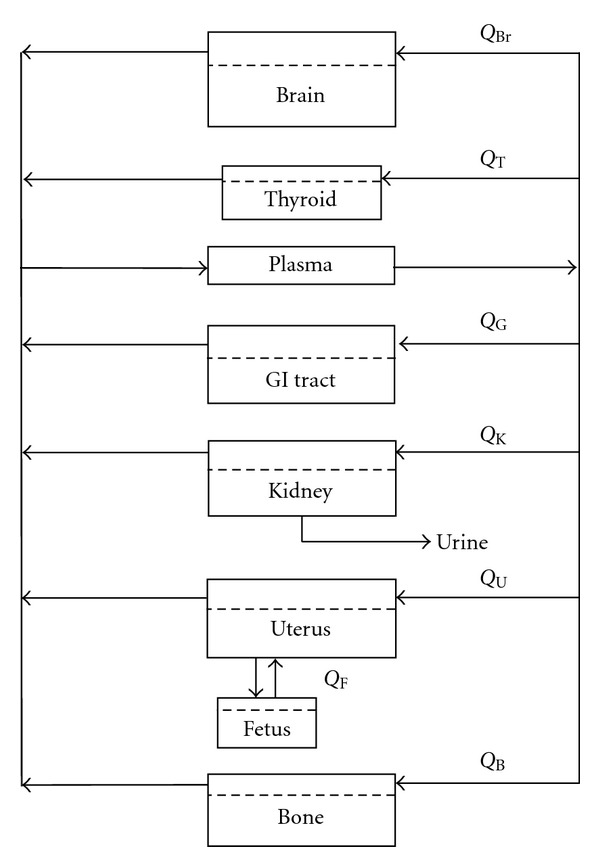
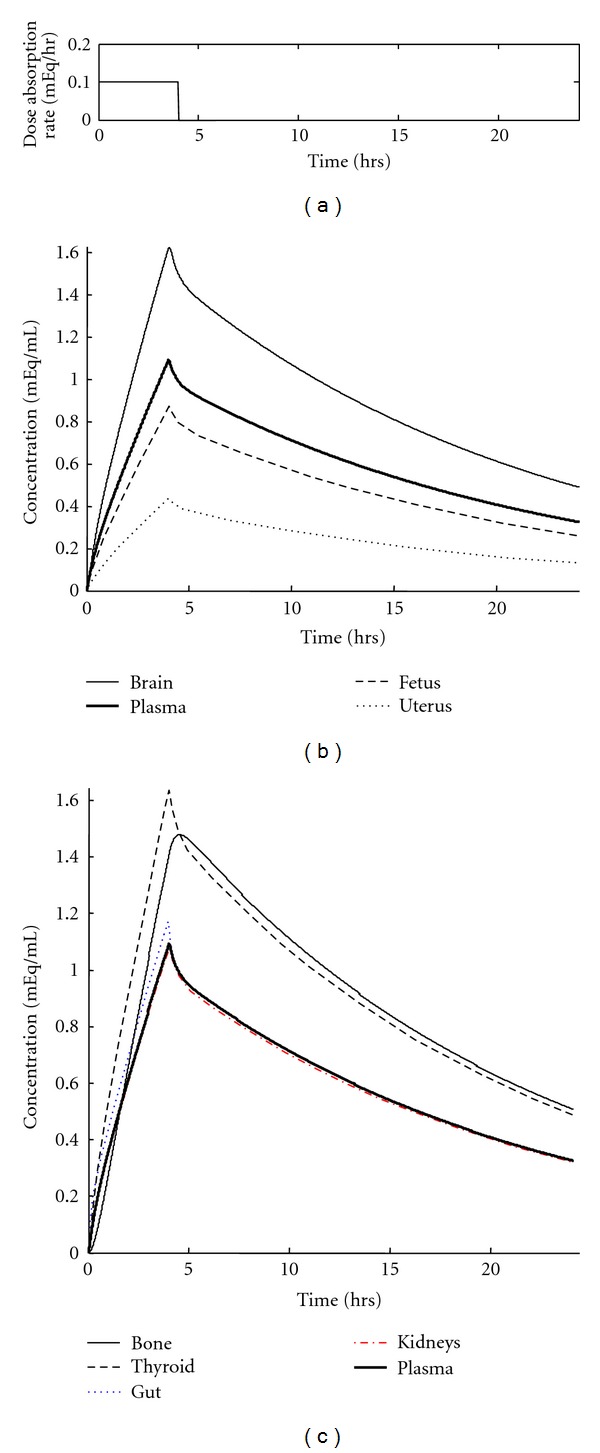
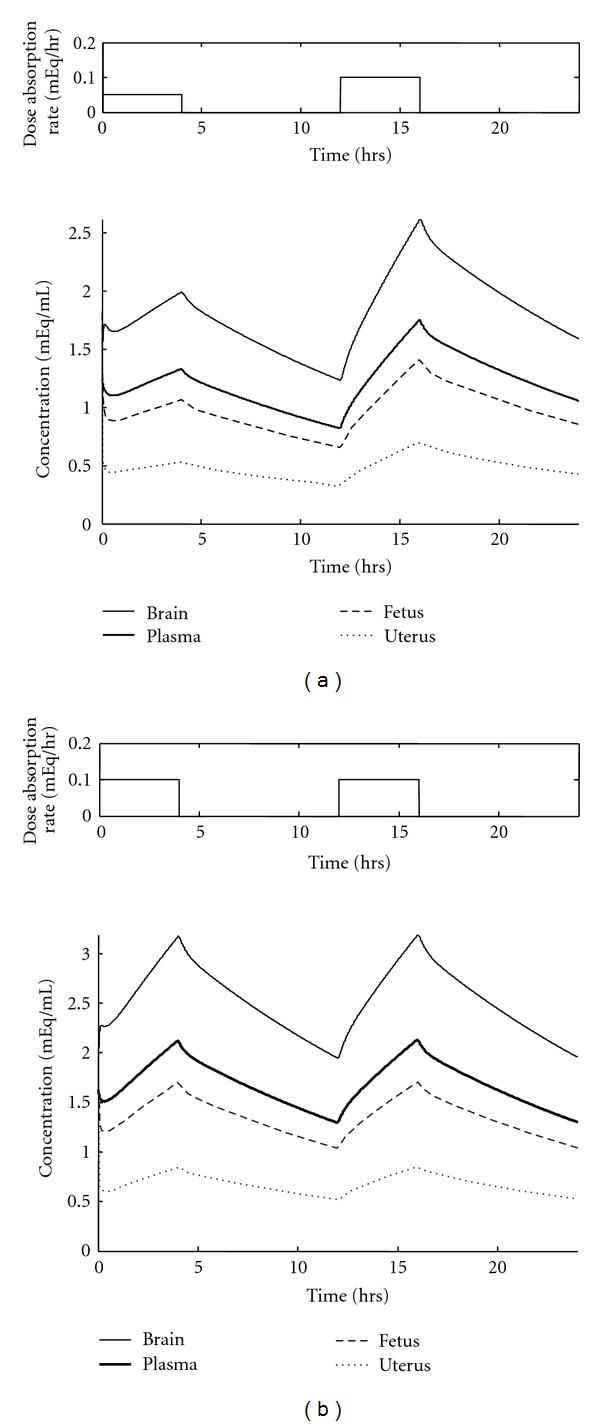
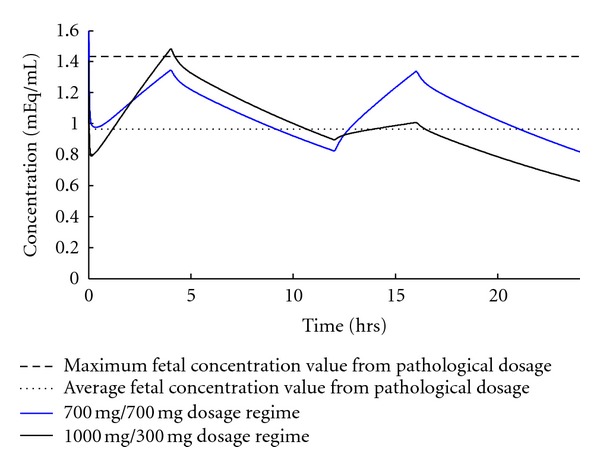
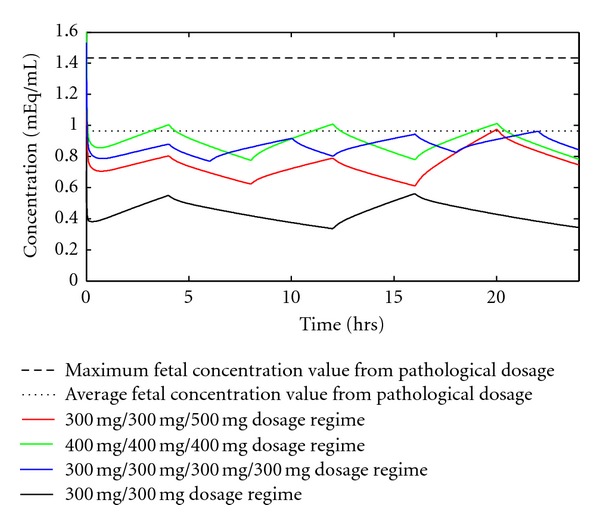
Treatment of bipolar disorder with lithium therapy during pregnancy is a medical challenge. Bipolar disorder is more prevalent in women and its onset is often concurrent with peak reproductive age. Treatment typically involves administration of the element lithium, which has been classified as a class D drug (legal to use during pregnancy, but may cause birth defects) and is one of only thirty known teratogenic drugs. There is no clear recommendation in the literature on the maximum acceptable dosage regimen for pregnant, bipolar women. We recommend a maximum dosage regimen based on a physiologically based pharmacokinetic (PBPK) model. The model simulates the concentration of lithium in the organs and tissues of a pregnant woman and her fetus. First, we modeled time-dependent lithium concentration profiles resulting from lithium therapy known to have caused birth defects. Next, we identified maximum and average fetal lithium concentrations during treatment. Then, we developed a lithium therapy regimen to maximize the concentration of lithium in the mother's brain, while maintaining the fetal concentration low enough to reduce the risk of birth defects. This maximum dosage regimen suggested by the model was 400 mg lithium three times per day.
Figures
References
-
- National Institute of Mental Health. NIH Publication. 09-3679. U.S. Department of Heath and Human Services, National Institutes of Health; 2009. Bipolar Disorder.
-
- Kozma C. Neonatal toxicity and transient neurodevelopmental deficits following prenatal exposure to lithium: another clinical report and a review of the literature. American Journal of Medical Genetics. 2005;132(4):441–444. - PubMed
-
- Lexi-Comp Online. Formulary and Drug Therapy Guide: Lithium. Hudson, Ohio, USA: Lexi-Comp; 2011.
-
- Blake LD, Lucas DN, Aziz K, Castello-Cortes A, Robinson PN. Lithium toxicity and the parturient: case report and literature review. International Journal of Obstetric Anesthesia. 2008;17(2):164–169. - PubMed
-
- Bendz H, Schön S, Attman PO, Aurell M. Renal failure occurs in chronic lithium treatment but is uncommon. Kidney International. 2010;77(3):219–224. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
