

Complications associated with liver transplantation in the obese recipient
- PMID: 22694047
- PMCID: PMC3518672
- DOI: 10.1111/j.1399-0012.2012.01669.x
Complications associated with liver transplantation in the obese recipient
Abstract
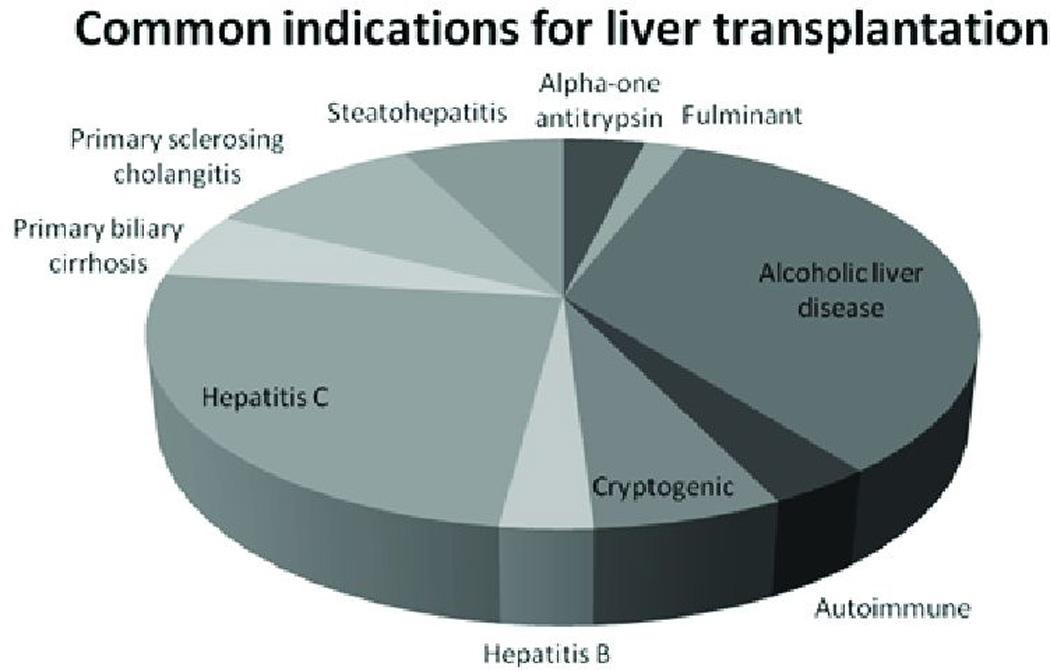
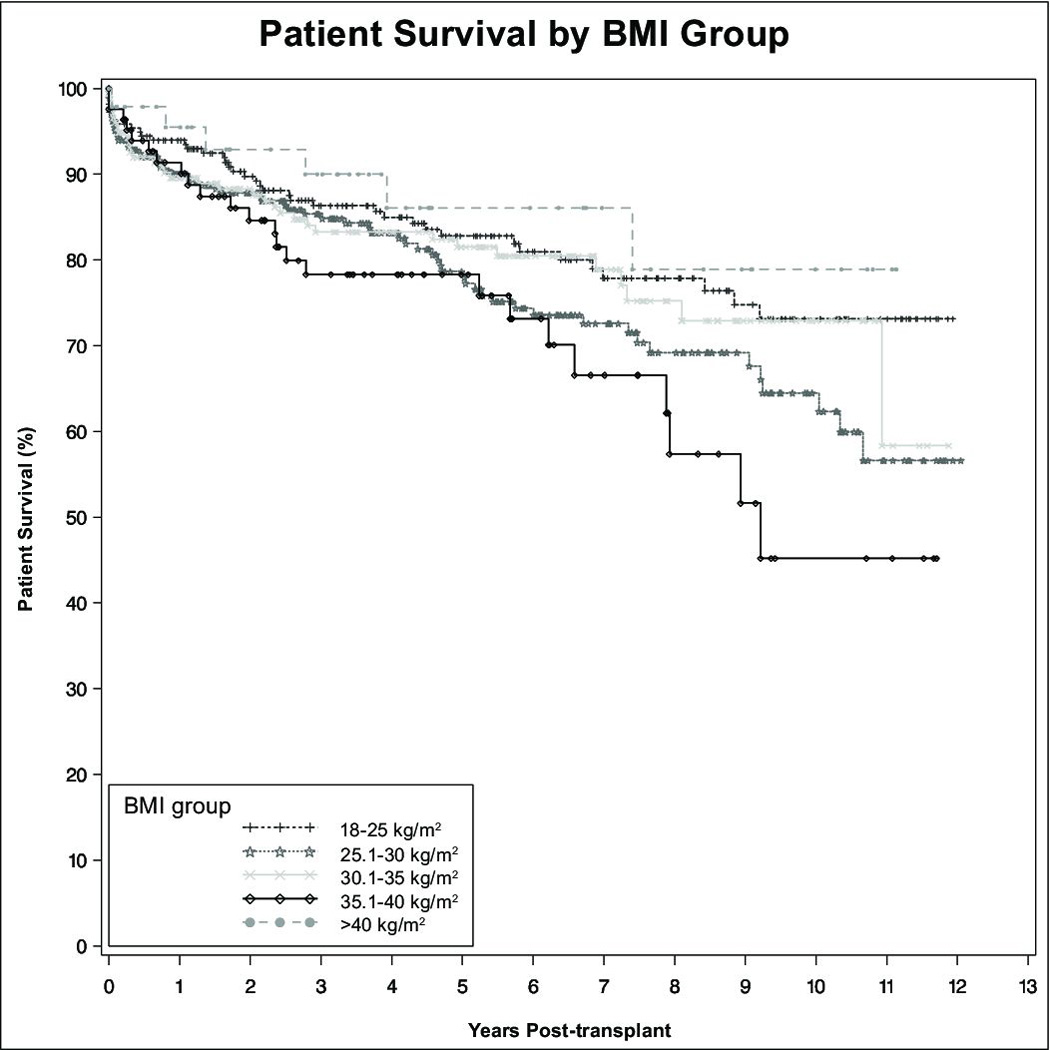
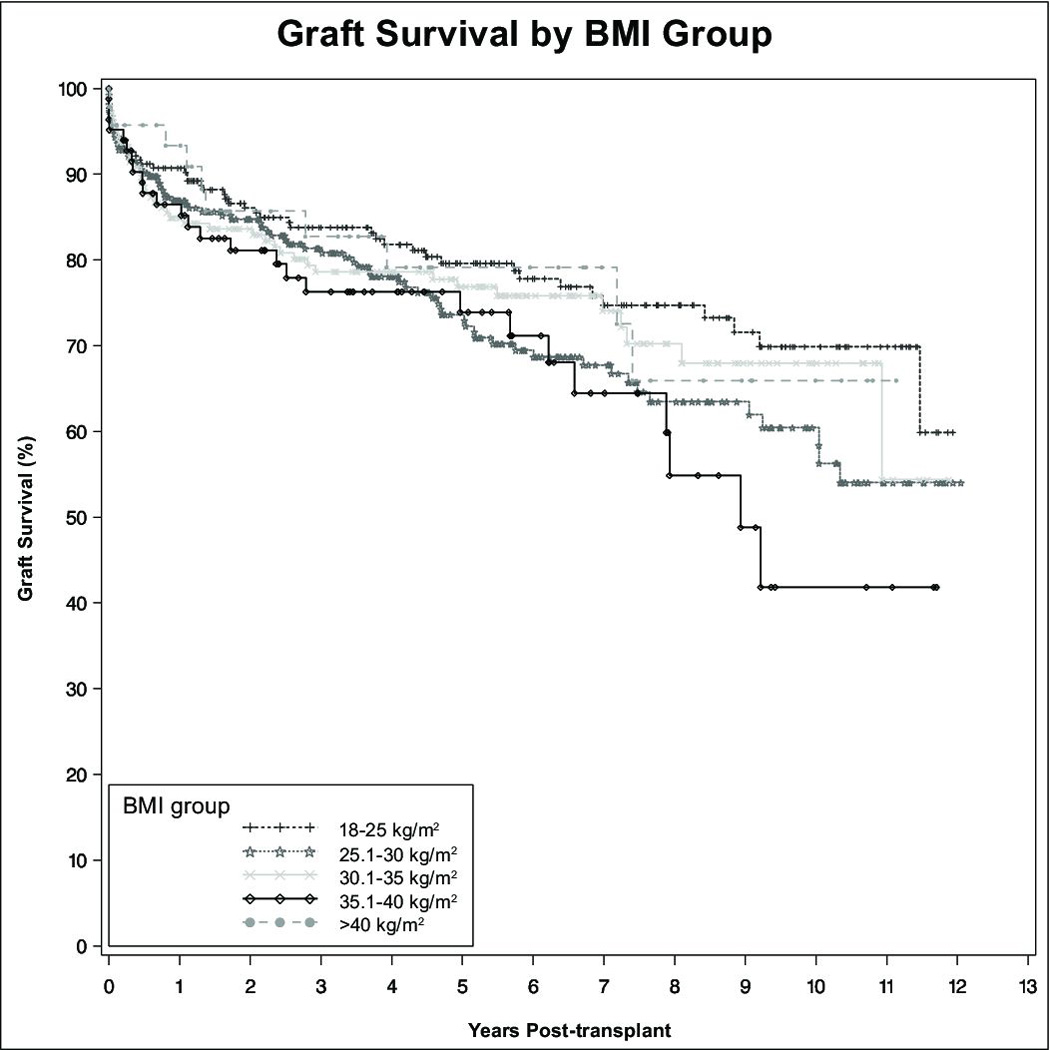
The prevalence of the metabolic syndrome with attendant morbid obesity continues to increase nationwide. A concomitant increase in non-alcoholic steatohepatitis (NASH) and associated end-stage liver disease requiring transplantation is expected to parallel this trend. Between January 1, 1997 and December 31, 2008, our center performed 813 solitary adult deceased-donor liver transplants. Patients were divided into groups based on the World Health Organization International Classification of obesity. Patients within each obesity class were compared to normal weight recipients. Preoperative demographics among all groups were similar. NASH was more common in higher BMI groups. Operative time, blood product usage, ICU length of stay, infectious complications, and biliary complications requiring intervention were all higher in obese recipients. Deep venous thrombosis occurred more commonly in patients with Class III obesity. Patients with Class II obesity had lower patient (HR 1.82, CI 1.09-3.01, p=0.02) and allograft survival (HR 1.62, CI 1.02-2.65, p=0.04). Obesity class did not reach statistical significance on multivariate analysis. Despite increased technical operative challenges and medical complexities associated with increasing recipient BMI, morbid obesity in and of itself should not be an absolute contraindication to liver transplantation as these patients have reasonable long-term outcomes.
© 2012 John Wiley & Sons A/S.
Figures
References
-
- Flegal KM. Epidemiologic aspects of overweight and obesity in the United States. Physiol Behav. 2005;86(5):599–602. - PubMed
-
- Charlton M. Nonalcoholic fatty liver disease: a review of current understanding and future impact. Clin Gastroenterol Hepatol. 2004;2(12):1048–1058. - PubMed
-
- Postlethwait RW, Johnson WD. Complications following surgery for duodenal ulcer in obese patients. Arch Surg. 1972;105(3):438–440. - PubMed
-
- Pemberton LB, Manax WG. Relationship of obesity to postoperative complications after cholecystectomy. Am J Surg. 1971;121(1):87–90. - PubMed
-
- Benoist S, et al. Impact of obesity on surgical outcomes after colorectal resection. Am J Surg. 2000;179(4):275–281. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
