

Complete steroid avoidance is effective and safe in children with renal transplants: a multicenter randomized trial with three-year follow-up
- PMID: 22694755
- PMCID: PMC3681527
- DOI: 10.1111/j.1600-6143.2012.04145.x
Complete steroid avoidance is effective and safe in children with renal transplants: a multicenter randomized trial with three-year follow-up
Abstract
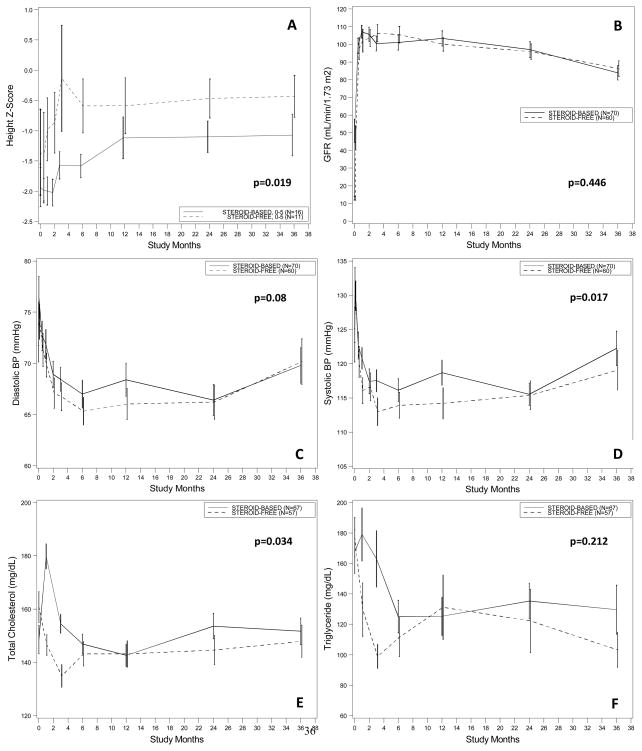
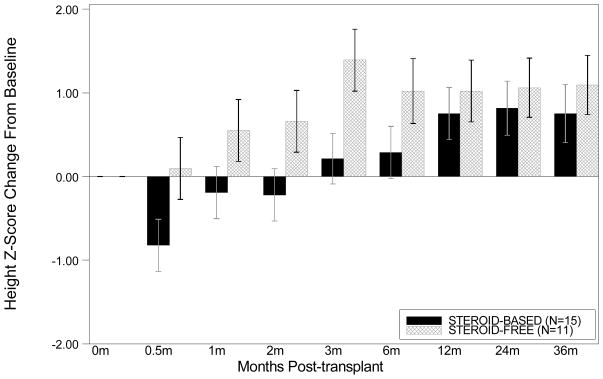
To determine whether steroid avoidance in pediatric kidney transplantation is safe and efficacious, a randomized, multicenter trial was performed in 12 pediatric kidney transplant centers. One hundred thirty children receiving primary kidney transplants were randomized to steroid-free (SF) or steroid-based (SB) immunosuppression, with concomitant tacrolimus, mycophenolate and standard dose daclizumab (SB group) or extended dose daclizumab (SF group). Follow-up was 3 years posttransplant. Standardized height Z-score change after 3 years follow-up was -0.99 ± 2.20 in SF versus -0.93 ± 1.11 in SB; p = 0.825. In subgroup analysis, recipients under 5 years of age showed improved linear growth with SF compared to SB treatment (change in standardized height Z-score at 3 years -0.43 ± 1.15 vs. -1.07 ± 1.14; p = 0.019). There were no differences in the rates of biopsy-proven acute rejection at 3 years after transplantation (16.7% in SF vs. 17.1% in SB; p = 0.94). Patient survival was 100% in both arms; graft survival was 95% in the SF and 90% in the SB arms (p = 0.30) at 3 years follow-up. Over the 3 year follow-up period, the SF group showed lower systolic BP (p = 0.017) and lower cholesterol levels (p = 0.034). In conclusion, complete steroid avoidance is safe and effective in unsensitized children receiving primary kidney transplants.
Trial registration: ClinicalTrials.gov NCT00141037.
© Copyright 2012 The American Society of Transplantation and the American Society of Transplant Surgeons.
Conflict of interest statement
None of the authors have any conflict of interest to declare in relation to this study.
Figures
Comment in
-
Transplantation: Steroid avoidance in pediatric transplant patients is safe.Nat Rev Nephrol. 2012 Jul 3;8(8):434. doi: 10.1038/nrneph.2012.130. Nat Rev Nephrol. 2012. PMID: 22751506 No abstract available.
References
-
- Goodwin WE, Mims MM, Kaufman JJ. Human renal transplantation. III. Technical problems encountered in six cases of kidney homotransplantation. J Urol. 1963 Mar;89:349–56. - PubMed
-
- Fine RN, Martz K, Stablein D. What have 20 years of data from the North American Pediatric Renal Transplant Cooperative Study taught us about growth following renal transplantation in infants, children, and adolescents with end-stage renal disease? Pediatr Nephrol. 2010 Apr;25(4):739–46. - PubMed
-
- Travis LB, Chesney R, McEnery P, Moel D, Pennisi A, Potter D, et al. Growth and glucocorticoids in children with kidney disease. Kidney Int. 1978 Oct;14(4):365–8. - PubMed
-
- Li L, Chaudhuri A, Weintraub LA, Hsieh F, Shah S, Alexander S, et al. Subclinical cytomegalovirus and Epstein-Barr virus viremia are associated with adverse outcomes in pediatric renal transplantation. Pediatr Transplant. 2007 Mar;11(2):187–95. - PubMed
-
- Knight SR, Morris PJ. Azathioprine and Steroids. In: Morris Peter, Knechtle Stuart., editors. Kidney Transplantation: Principles and Practice. 6. Philadelphia: W.B. Saunders; 2008. pp. 220–33.
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
