

Persistent inflammation and immunosuppression: a common syndrome and new horizon for surgical intensive care
- PMID: 22695412
- PMCID: PMC3705923
- DOI: 10.1097/TA.0b013e318256e000
Persistent inflammation and immunosuppression: a common syndrome and new horizon for surgical intensive care
Abstract
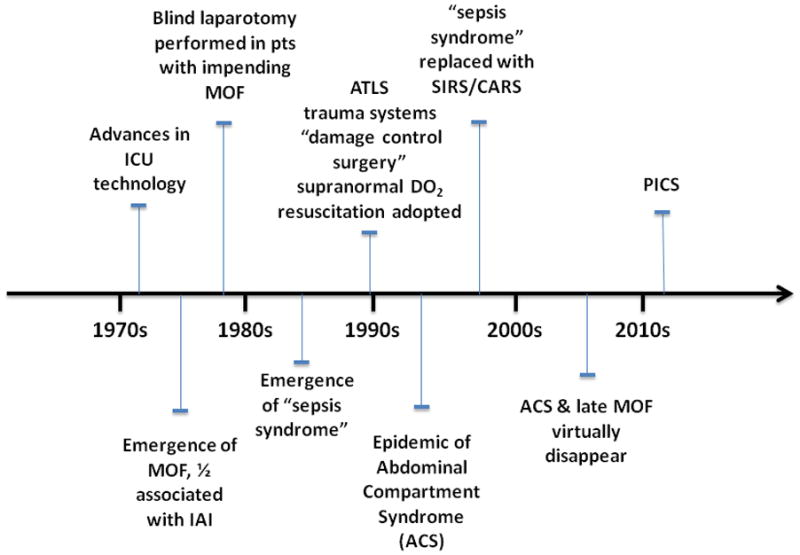
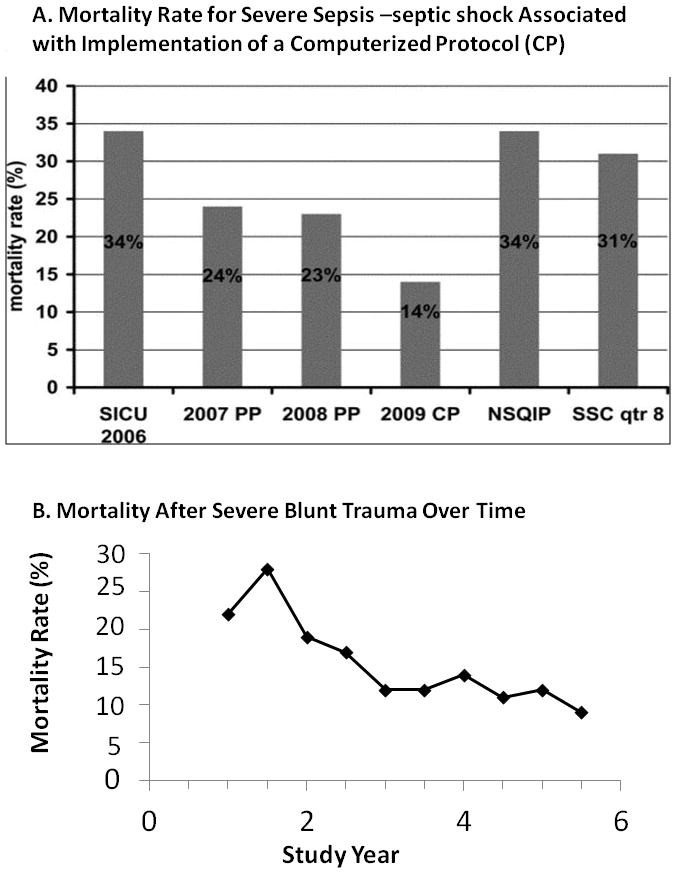
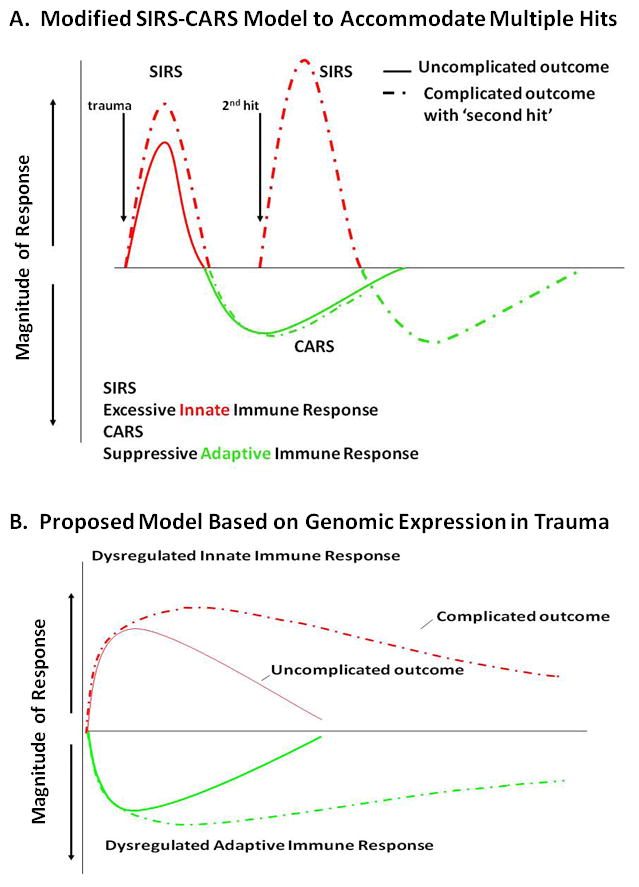
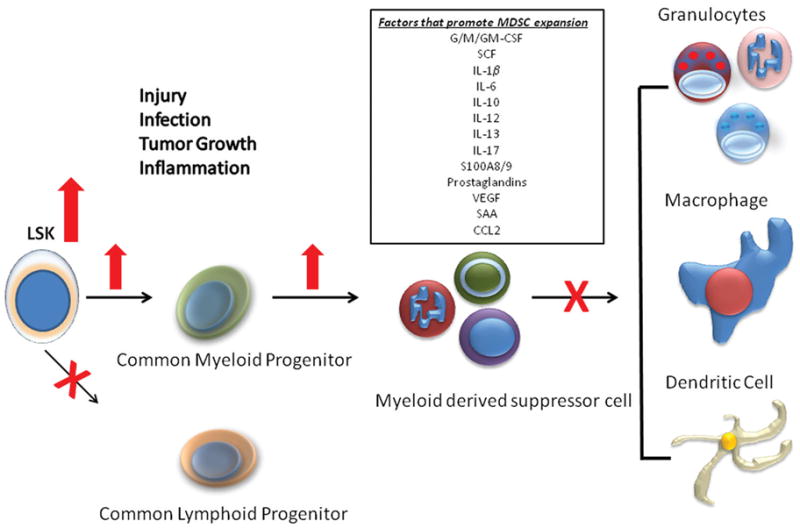
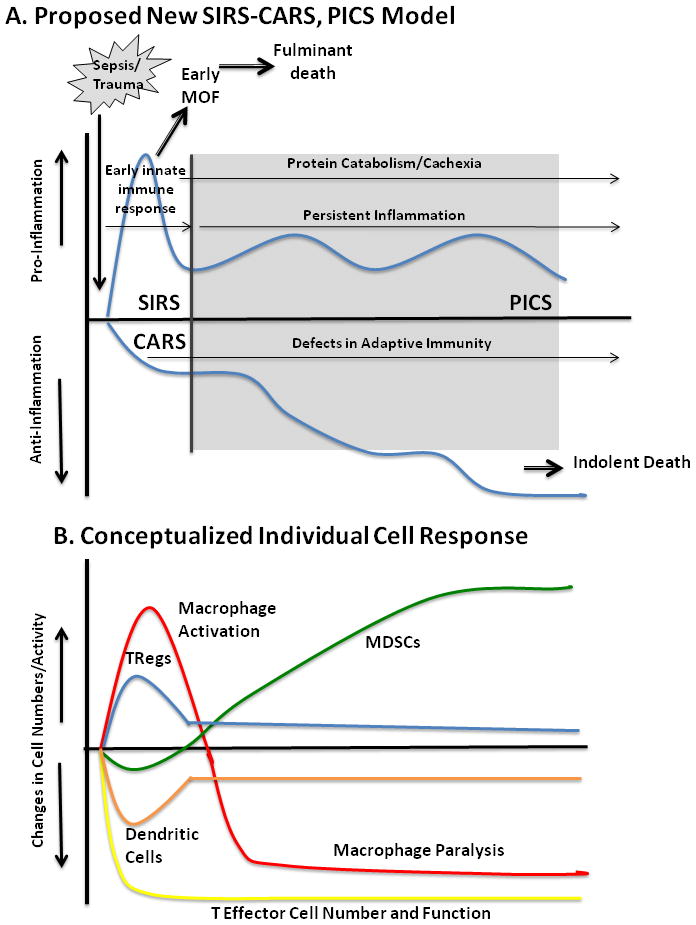
Surgical intensive care unit (ICU) stay of longer than 10 days is often described by the experienced intensivist as a "complicated clinical course" and is frequently attributed to persistent immune dysfunction. "Systemic inflammatory response syndrome" (SIRS) followed by "compensatory anti-inflammatory response syndrome" (CARS) is a conceptual framework to explain the immunologic trajectory that ICU patients with severe sepsis, trauma, or emergency surgery for abdominal infection often traverse, but the causes, mechanisms, and reasons for persistent immune dysfunction remain unexplained. Often involving multiple-organ failure (MOF) and death, improvements in surgical intensive care have altered its incidence, phenotype, and frequency and have increased the number of patients who survive initial sepsis or surgical events and progress to a persistent inflammation, immunosuppression, and catabolism syndrome (PICS). Often observed, but rarely reversible, these patients may survive to transfer to a long-term care facility only to return to the ICU, but rarely to self-sufficiency. We propose that PICS is the dominant pathophysiology and phenotype that has replaced late MOF and prolongs surgical ICU stay, usually with poor outcome. This review details the evolving epidemiology of MOF, the clinical presentation of PICS, and our understanding of how persistent inflammation and immunosuppression define the pathobiology of prolonged intensive care. Therapy for PICS will involve innovative interventions for immune system rebalance and nutritional support to regain physical function and well-being.
Copyright © 2012 by Lippincott Williams & Wilkins.
Conflict of interest statement
Conflict of Interest Statement: No conflict of interests have been declared.
Figures
References
-
- Moore FA, Moore EE. Evolving concepts in the pathogenesis of postinjury multiple organ failure. Surg Clin North Am. 1995;75(2):257–77. - PubMed
-
- Waydhas C, Nast-Kolb D, Jochum M, Trupka A, Lenk S, Fritz H, Duswald KH, Schweiberer L. Inflammatory mediators, infection, sepsis, and multiple organ failure after severe trauma. Arch Surg. 1992;127(4):460–7. - PubMed
-
- Nuytinck HK, Offermans XJ, Kubat K, Goris RJ. Whole body inflammation in trauma patients; an autopsy study. Prog Clin Biol Res. 1987;236A:55–61. - PubMed
-
- Faist E, Baue AE, Dittmer H, Heberer G. Multiple organ failure in polytrauma patients. J Trauma. 1983;23(9):775–87. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
