

Community falls prevention for people who call an emergency ambulance after a fall: an economic evaluation alongside a randomised controlled trial
- PMID: 22695789
- PMCID: PMC3424053
- DOI: 10.1093/ageing/afs071
Community falls prevention for people who call an emergency ambulance after a fall: an economic evaluation alongside a randomised controlled trial
Abstract
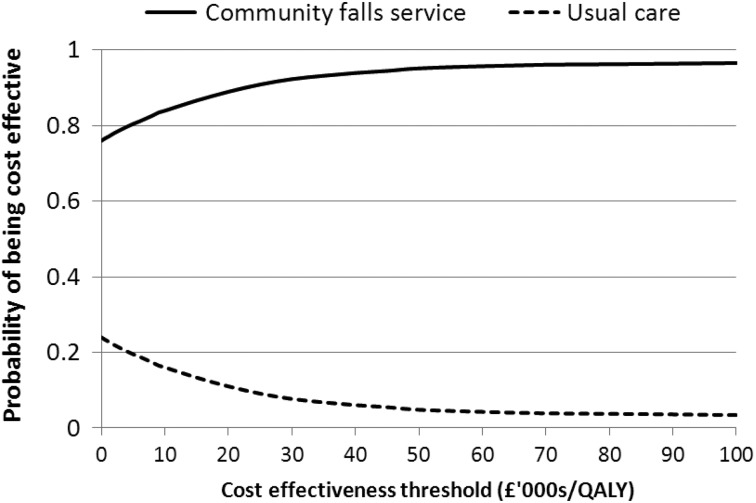
Objective: we estimated the cost-effectiveness of a community falls prevention service compared with usual care from a National Health Service and personal social services perspective over the 12 month trial period.
Design: a cost-effectiveness and cost utility analysis alongside a randomised controlled trial
Setting: community.
Participants: people over 60 years of age living at home or in residential care who had fallen and called an emergency ambulance but were not taken to hospital.
Interventions: referral to community fall prevention services or usual health and social care.
Measurements: incremental cost per fall prevented and incremental cost per Quality-Adjusted Life Years (QALYs)
Results: a total of 157 participants (82 interventions and 75 controls) were used to perform the economic evaluation. The mean difference in NHS and personal social service costs between the groups was £-1,551 per patient over 1 year (95% CI: £-5,932 to £2,829) comparing the intervention and control groups. The intervention patients experienced on average 5.34 fewer falls over 12 months (95% CI: -7.06 to -3.62). The mean difference in QALYs was 0.070 (95% CI: -0.010 to 0.150) in favour of the intervention group.
Conclusion: the community falls prevention service was estimated to be cost-effective in this high-risk group. Current Controlled Trials ISRCTN67535605. (controlled-trials.com).
Figures
References
-
- Tinetti M, Speechley M, Ginter S. Risk factors for falls among elderly persons living within the community. N Engl J Med. 1988;319:1701–7. - PubMed
-
- Gillespie LD, Robertson MC, Gillespie WJ, et al. Interventions for preventing falls in older people living in the community. Cochrane Database Syst Rev. 2009;2:CD007146. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
