

MRI of the lung (2/3). Why … when … how?
- PMID: 22695944
- PMCID: PMC3481084
- DOI: 10.1007/s13244-011-0146-8
MRI of the lung (2/3). Why … when … how?
Abstract
Background: Among the modalities for lung imaging, proton magnetic resonance imaging (MRI) has been the latest to be introduced into clinical practice. Its value to replace X-ray and computed tomography (CT) when radiation exposure or iodinated contrast material is contra-indicated is well acknowledged: i.e. for paediatric patients and pregnant women or for scientific use. One of the reasons why MRI of the lung is still rarely used, except in a few centres, is the lack of consistent protocols customised to clinical needs.
Methods: This article makes non-vendor-specific protocol suggestions for general use with state-of-the-art MRI scanners, based on the available literature and a consensus discussion within a panel of experts experienced in lung MRI.
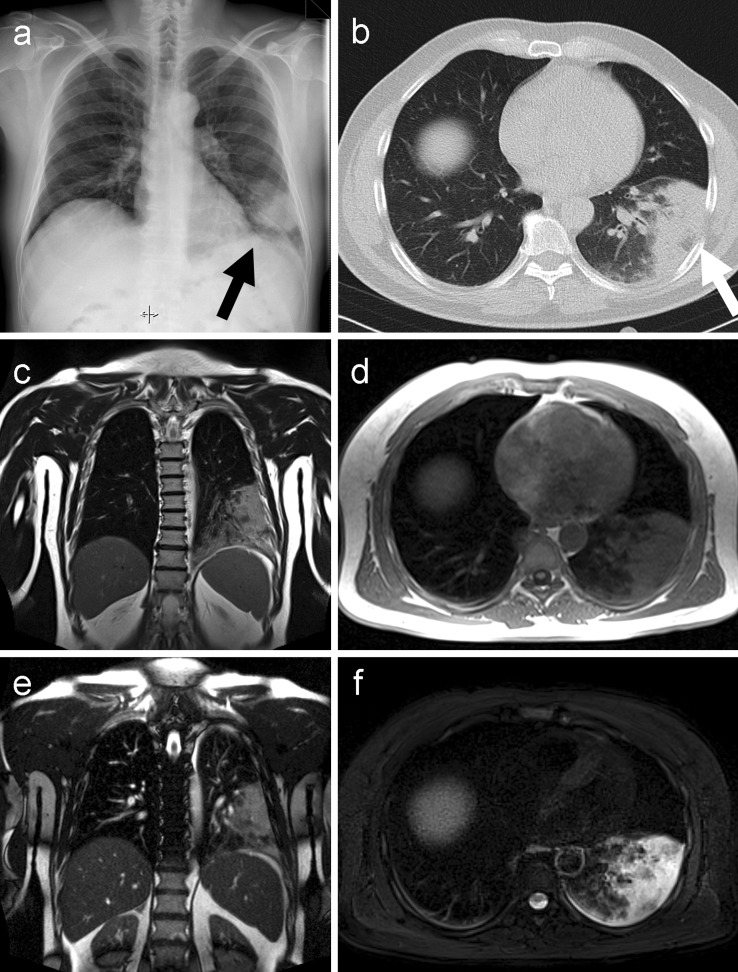
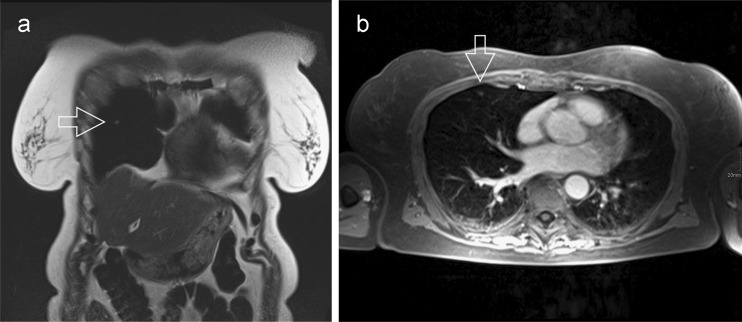
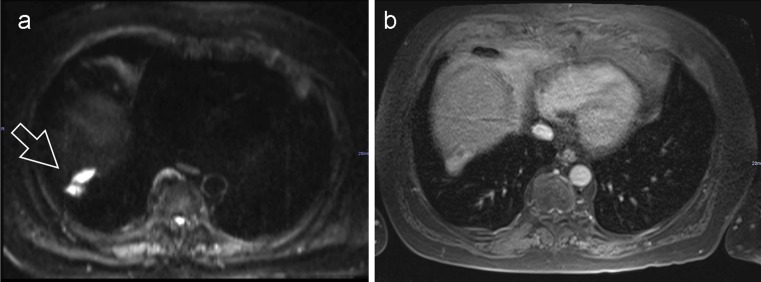
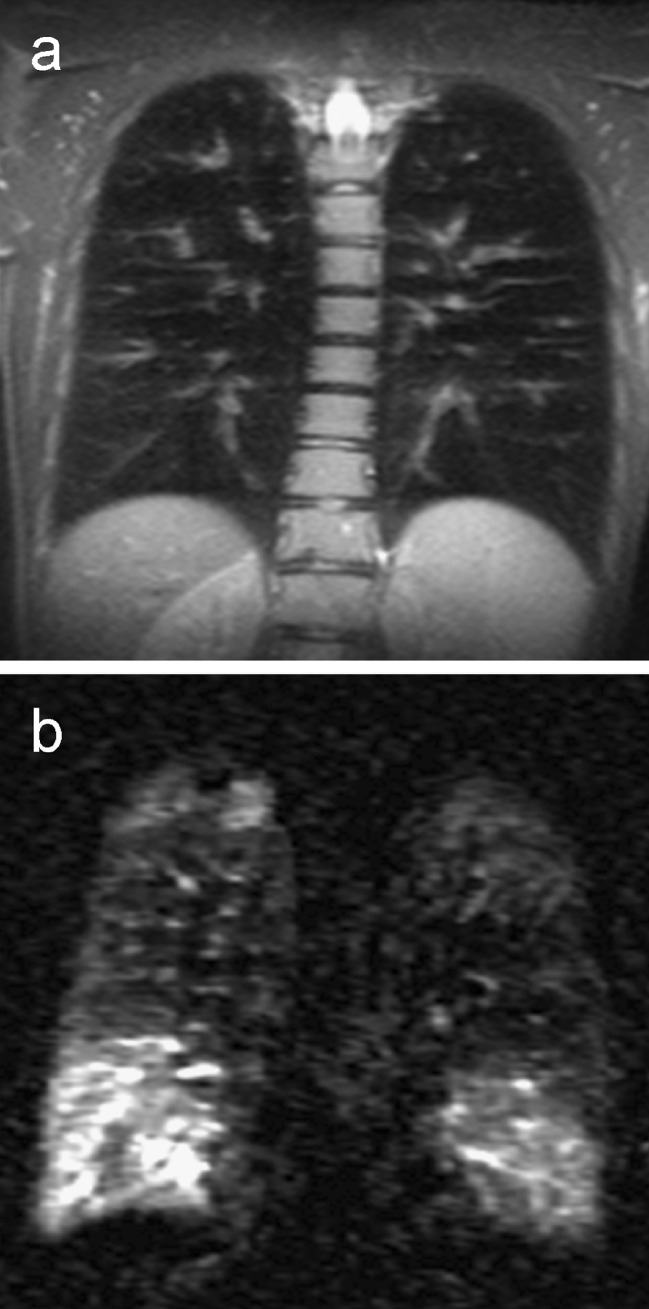
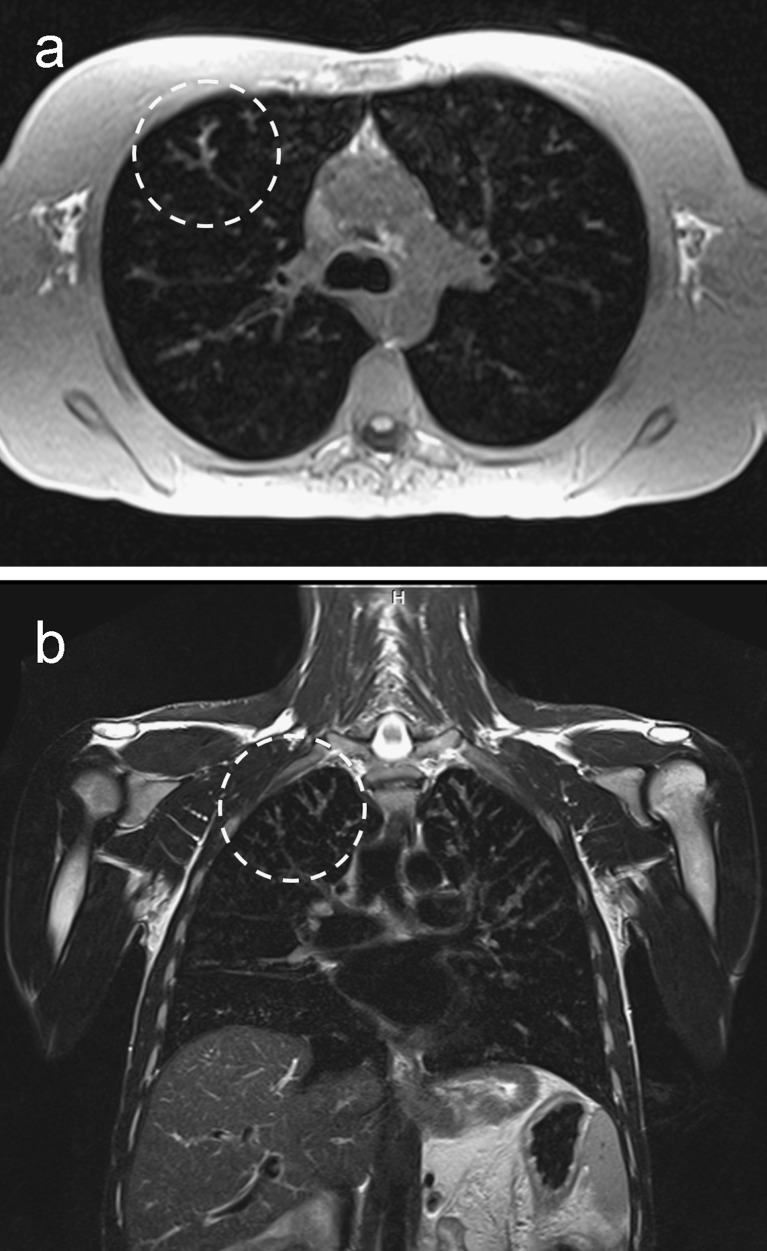
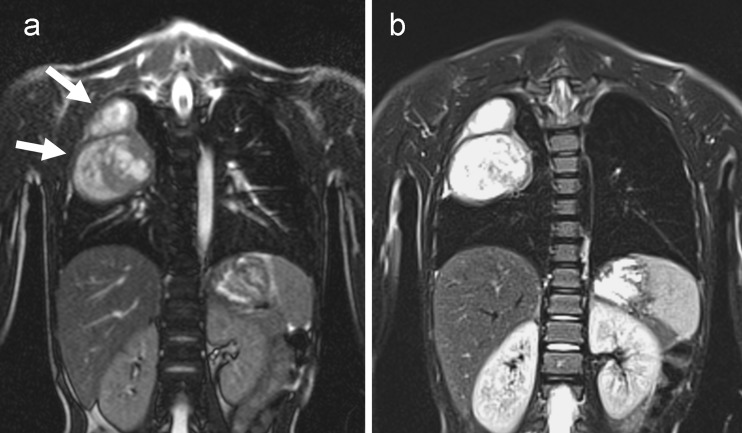
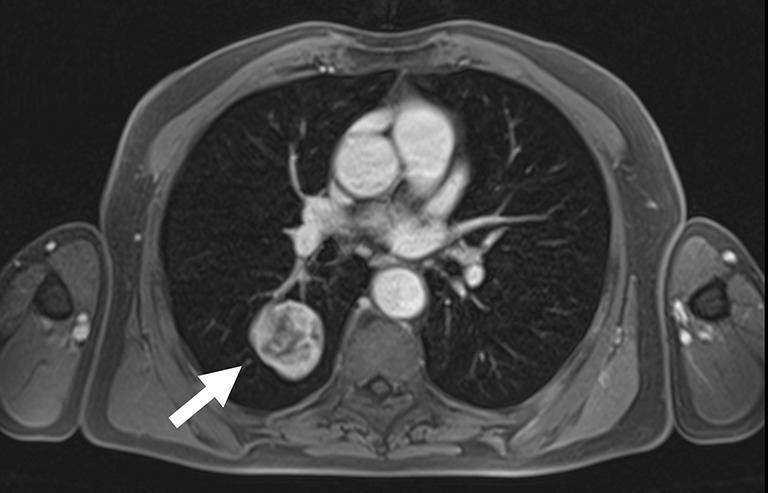
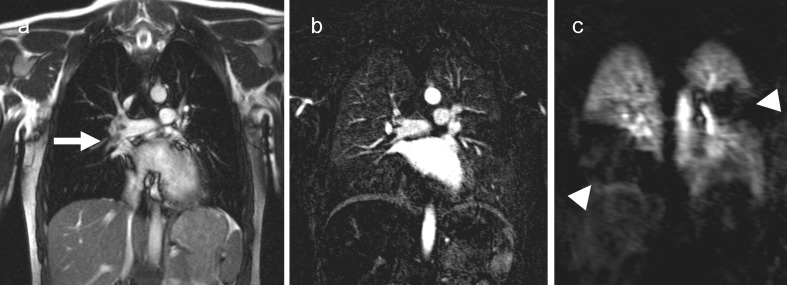
Results: Various sequences have been successfully tested within scientific or clinical environments. MRI of the lung with appropriate combinations of these sequences comprises morphological and functional imaging aspects in a single examination. It serves in difficult clinical problems encountered in daily routine, such as assessment of the mediastinum and chest wall, and even might challenge molecular imaging techniques in the near future.
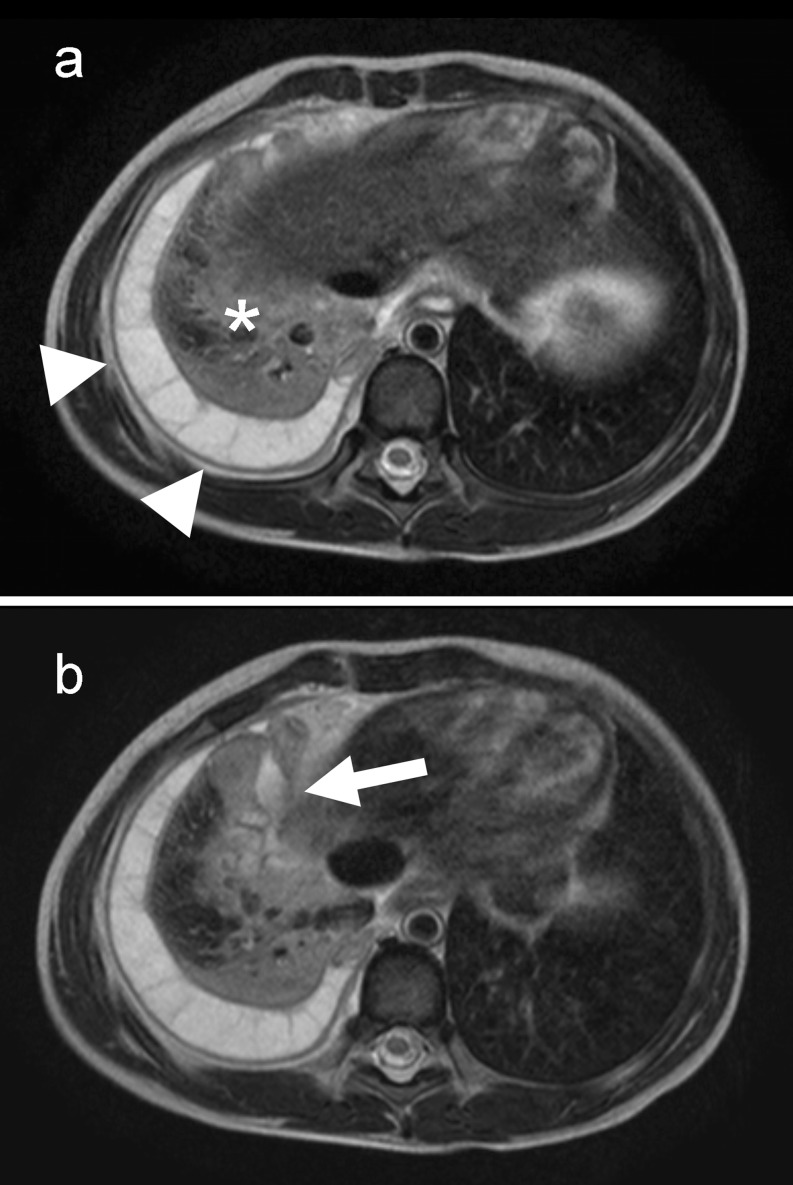
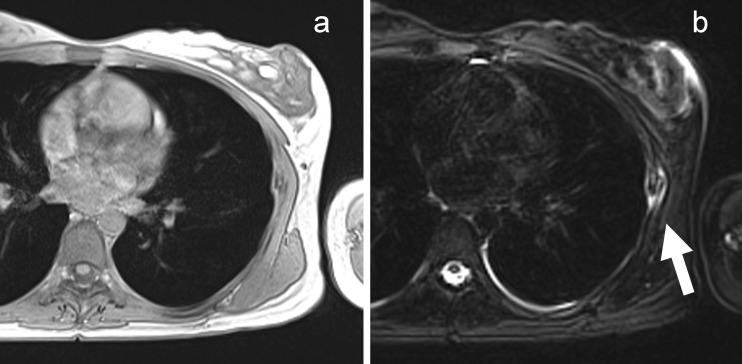
Conclusion: This article helps new users to implement appropriate protocols on their own MRI platforms. Main Messages • MRI of the lung can be readily performed on state-of-the-art 1.5-T MRI scanners. • Protocol suggestions based on the available literature facilitate its use for routine • MRI offers solutions for complicated thoracic masses with atelectasis and chest wall invasion. • MRI is an option for paediatrics and science when CT is contra-indicated.
Figures
References
-
- Biederer J, Bauman G, Hintze C, Fabel M, Both M. Magnetresonanztomographie. Der Pneumologe. 2011;8:234–242. doi: 10.1007/s10405-010-0440-z. - DOI
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
