

Paediatric multi-detector row chest CT: what you really need to know
- PMID: 22696085
- PMCID: PMC3369117
- DOI: 10.1007/s13244-012-0152-5
Paediatric multi-detector row chest CT: what you really need to know
Abstract
Background: The emergence of multi-detector row CT (MDCT) has established and extended the role of CT especially in paediatric chest imaging. This has altered the way in which data is acquired and is perceived as the 'gold standard' in the detection of certain chest pathologies. The range of available post-processing tools provide alternative ways in which CT images can be manipulated for review and interpretation in order to enhance diagnostic accuracy.
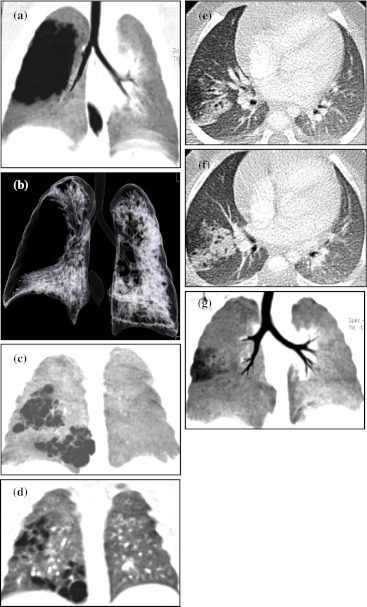
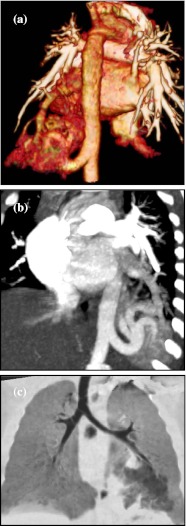
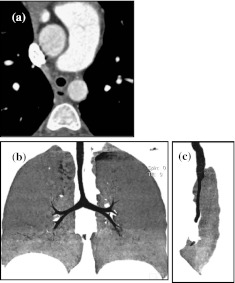
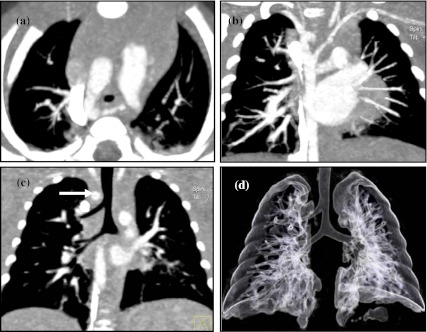
Methodology: Paediatric imaging technique/protocol together with radiation dose reduction is discussed in detail. The use of different post-processing tools to best demonstrate the wide range of important congenital anomalies and thoracic pathologies is outlined and presented pictorially.
Conclusion: MDCT with its isotropic resolution and fast imaging acquisition times reduces the need for invasive diagnostic investigations. However, users must be vigilant in their imaging techniques to minimise radiation burden, whilst maintaining good image quality. Main Messages • CT examinations should be clinically justified by the referring clinician and radiologist. • MDCT is invaluable for evaluating the central airway, mediastinal structures and lung parenchyma. • MDCT is more sensitive than plain radiographs in detection of structural changes within the lungs.
Figures











References
LinkOut - more resources
Full Text Sources
