

Caesarean section versus vaginal delivery for preterm birth in singletons
- PMID: 22696314
- PMCID: PMC4164504
- DOI: 10.1002/14651858.CD000078.pub2
Caesarean section versus vaginal delivery for preterm birth in singletons
Update in
-
Caesarean section versus vaginal delivery for preterm birth in singletons.Cochrane Database Syst Rev. 2013 Sep 12;2013(9):CD000078. doi: 10.1002/14651858.CD000078.pub3. Cochrane Database Syst Rev. 2013. PMID: 24030708 Free PMC article.
Abstract
Background: Planned caesarean delivery for women thought be in preterm labour may be protective for baby, but could also be quite traumatic for both mother and baby. The optimal mode of delivery of preterm babies for both cephalic and breech presentation remains, therefore, controversial.
Objectives: To assess the effects of a policy of planned immediate caesarean delivery versus planned vaginal birth for women in preterm labour.
Search methods: We searched the Cochrane Pregnancy and Childbirth Group's Trials Register (24 April 2012).
Selection criteria: Randomised trials comparing a policy of planned immediate caesarean delivery versus planned vaginal delivery for preterm birth.
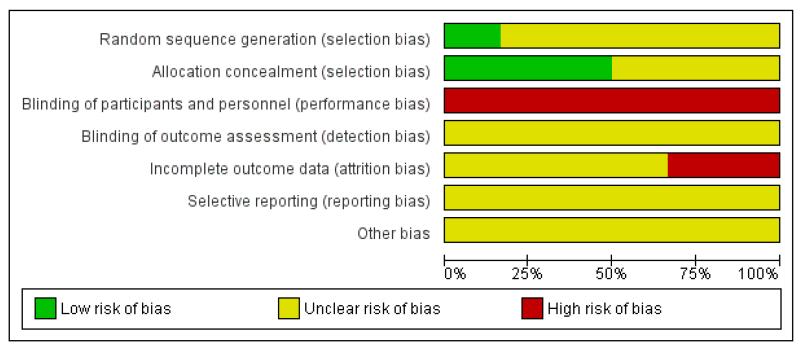
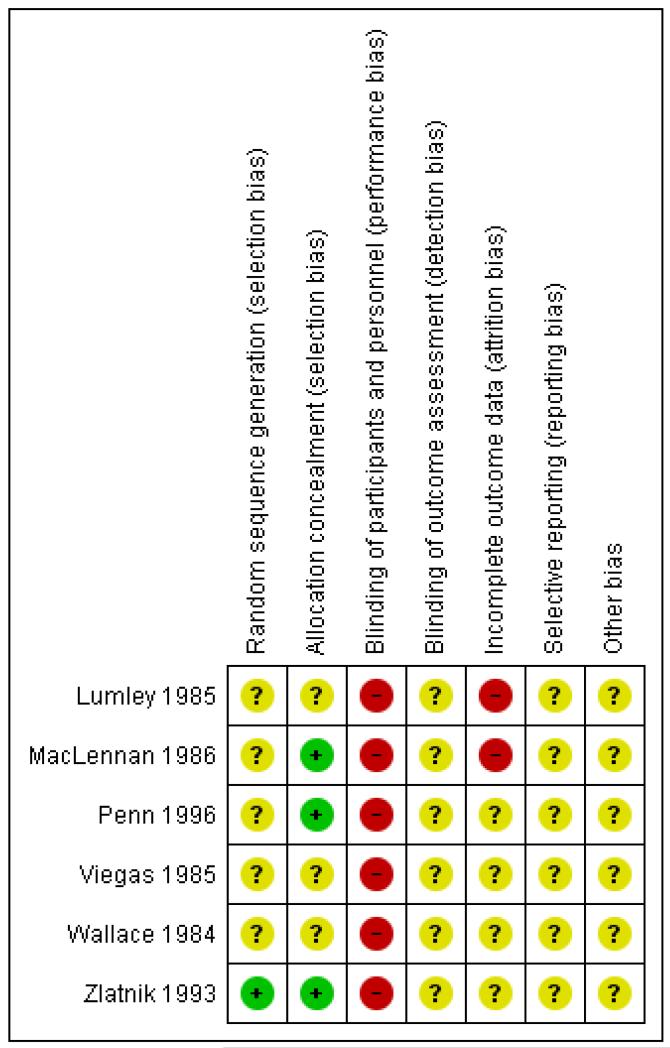
Data collection and analysis: Two review authors independently assessed trials for inclusion. Two review authors independently extracted data and assessed risk of bias. Data were checked for accuracy.
Main results: We included six studies (involving 122 women) but only four studies (involving only 116 women) contributed data to the analyses.Infant There were very little data of relevance to the three main (primary) outcomes considered in this review: There was no significant difference between planned immediate caesarean section and planned vaginal delivery with respect to birth injury to infant (risk ratio (RR) 0.56, 95%, confidence interval (CI) 0.05 to 5.62; one trial, 38 women) or birth asphyxia (RR 1.63, 95% CI 0.84 to 3.14; one trial, 12 women). The only cases of birth trauma were a laceration of the buttock in a baby who was delivered by caesarean section and mild bruising in another allocated to the group delivered vaginally.The difference between the two groups with regard to perinatal deaths was not significant (0.29, 95% CI 0.07 to 1.14; three trials, 89 women) and there were no data specifically relating to neonatal admission to special care and/or intensive care unit.There was also no difference between the caesarean or vaginal delivery groups in terms of markers of possible birth asphyxia (RR 1.63, 95% CI 0.84 to 3.14; one trial, 12 women) or Apgar score less than seven at five minutes (RR 0.83, 95% CI 0.43 to 1.60; four trials, 115 women) and no difference in attempts at breastfeeding (RR 1.40, 95% 0.11 to 17.45; one trial, 12 women). There was also no difference in neonatal fitting/seizures (RR 0.22, 95% CI 0.01 to 4.32; three trials, 77 women), hypoxic ischaemic encephalopathy (RR 4.00, 95% CI 0.20 to 82.01;one trial, 12 women) or respiratory distress syndrome (RR 0.55, 95% CI 0.27 to 1.10; three trials, 103 women). There were no data reported in the trials specifically relating to meconium aspiration. There was also no significant difference between the two groups for abnormal follow-up in childhood (RR 0.65, 95% CI 0.19 to 2.22; one trial, 38 women) or delivery less than seven days after entry (RR 0.95, 95% CI 0.73 to 1.24; two trials, 51 women). Mother: There were no data reported on maternal admissions to intensive care. However, there were seven cases of major maternal postpartum complications in the group allocated to planned immediate caesarean section and none in the group randomised to vaginal delivery (RR 7.21, 95% CI 1.37 to 38.08; four trials, 116 women).There were no data reported in the trials specifically relating to maternal satisfaction (postnatal). There was no significant difference between the two groups with regard to postpartum haemorrhage. A number of non-prespecified secondary outcomes were also considered in the analyses. There was a significant advantage for women in the vaginal delivery group with respect to maternal puerperal pyrexia (RR 2.98, 95% CI 1.18 to 7.53; three trials, 89 women) and other maternal infection (RR 2.63, 95% CI 1.02 to 6.78; three trials, 103 women), but no significant differences in wound infection (RR 1.16, 95% CI 0.18 to 7.70; three trials, 103 women), maternal stay more than 10 days (RR 1.27, 95% CI 0.35 to 4.65; three trials, 78 women) or the need for blood transfusion (results not estimable).
Authors' conclusions: There is not enough evidence to evaluate the use of a policy of planned immediate caesarean delivery for preterm babies. Further studies are needed in this area, but recruitment is proving difficult.
Figures
Update of
-
Elective caesarean section versus expectant management for delivery of the small baby.Cochrane Database Syst Rev. 2001;(2):CD000078. doi: 10.1002/14651858.CD000078. Cochrane Database Syst Rev. 2001. Update in: Cochrane Database Syst Rev. 2012 Jun 13;(6):CD000078. doi: 10.1002/14651858.CD000078.pub2. PMID: 11405950 Updated.
References
References to studies included in this review
-
- Lumley J, Lester A, Renou P, Wood C. A failed RCT to determine the best method of delivery for very low birth weight infants. Controlled Clinical Trials. 1985;6:120–7. - PubMed
-
- MacLennan AH. Randomised trial of the mode of delivery of the very premature infant (trial abandoned) Personal communication. 1986 Oct 28th;
-
- Penn ZJ, Steer PJ, Grant AM. A multicentre randomised controlled trial comparing elective and selective caesarean section for the delivery of the preterm breech infant. British Journal of Obstetrics and Gynaecology. 1996;103(7):684–9. - PubMed
-
- Viegas OAC, Ingemarsson I, Sim LP, Singh K, Cheng M, Ratnam SS, et al. Collaborative study on preterm breeches: vaginal delivery versus caesarean section. Asia Oceania Journal of Obstetrics and Gynaecology. 1985;11:349–55. - PubMed
-
- Wallace RL, Schifrin BS, Paul RH. The delivery route for very-low-birth-weight infants. Journal of Reproductive Medicine. 1984;29:736–40. - PubMed
References to studies excluded from this review
-
- Dietl J. Effect of delivery route on outcome of infants at early gestational age. Personal communication. 1987
-
- McColgin S. Delivery of the vertex VLBW infant: vaginal vs Caesarean section delivery. Personal communication. 1990
Additional references
-
- Cohen M, Carson BS. Respiratory morbidity benefit of awaiting onset of labor after elective cesarean section. Obstetrics & Gynecology. 1985;65(6):818–24. - PubMed
-
- Doyle LW, Crowther CA, Middleton P, Marret S, Rouse D. Magnesium sulphate for women at risk of preterm birth for neuroprotection of the fetus. Cochrane Database of Systematic Reviews. 2009;(Issue 1) [DOI: 10.1002/14651858.CD004661.pub3] - PubMed
-
- Department of Health. Welsh Office. Scottish Office Department of Health. Department of Health and Social Services NI . In: Report on Confidential Enquiries into Maternal Deaths in the United Kingdom. Rubery E, Bourdillon P, Hibbard B, editors. HMSO; London: 1996.
-
- Gravenhorst JB, Schreuder AM, Veen S, Brand R, Verloove-Vanhorick SP, Verweij RA, et al. Breech delivery in very preterm and very low birthweight infants in The Netherlands. British Journal of Obstetrics and Gynaecology. 1993;100(5):411–5. - PubMed
References to other published versions of this review
-
- Grant A. Elective or selective caesarean section of the small baby? A systematic review of the controlled trials. British Journal of Obstetrics and Gynaecology. 1996;103(12):1197–200. - PubMed
-
- Grant A. Elective versus selective caesarean section for delivery of the small baby. Cochrane Database of Systematic Reviews. 2000;(Issue 4) - PubMed
-
- Grant A. Elective versus selective caesarean section for delivery of the small baby. Cochrane Database of Systematic Reviews. 2001;(Issue 1) - PubMed
-
- Grant A, Glazer CMA. Elective caesarean section versus expectant management for delivery of the small baby. Cochrane Database of Systematic Reviews. 2010;(Issue 2) [DOI: 10.1002/14651858.CD000078] - PubMed
-
-
* Indicates the major publication for the study
-
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous