

Induction of labour for improving birth outcomes for women at or beyond term
- PMID: 22696345
- PMCID: PMC4065650
- DOI: 10.1002/14651858.CD004945.pub3
Induction of labour for improving birth outcomes for women at or beyond term
Update in
-
Induction of labour for improving birth outcomes for women at or beyond term.Cochrane Database Syst Rev. 2018 May 9;5(5):CD004945. doi: 10.1002/14651858.CD004945.pub4. Cochrane Database Syst Rev. 2018. Update in: Cochrane Database Syst Rev. 2020 Jul 15;7:CD004945. doi: 10.1002/14651858.CD004945.pub5. PMID: 29741208 Free PMC article. Updated.
Abstract
Background: As a pregnancy continues beyond term the risks of babies dying inside the womb or in the immediate newborn period increase. Whether a policy of labour induction at a predetermined gestational age can reduce this increased risk is the subject of this review.
Objectives: To evaluate the benefits and harms of a policy of labour induction at term or post-term compared with awaiting spontaneous labour or later induction of labour.
Search methods: We searched the Cochrane Pregnancy and Childbirth Group's Trials Register (31 March 2012).
Selection criteria: Randomised controlled trials conducted in women at or beyond term. The eligible trials were those comparing a policy of labour induction with a policy of awaiting spontaneous onset of labour. Cluster-randomised trials and cross-over trials are not included. Quasi-random allocation schemes such as alternation, case record numbers or open random-number lists were not eligible.
Data collection and analysis: Two review authors independently assessed trials for inclusion. Two review authors independently assessed trial quality and extracted data. Data were checked for accuracy. Outcomes are analysed in two main categories: gestational age and cervix status.
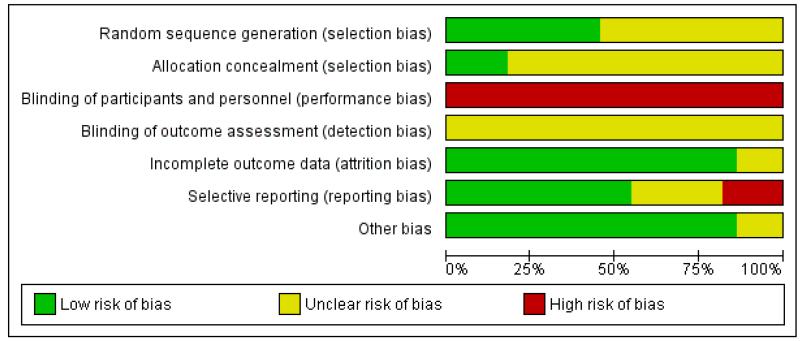
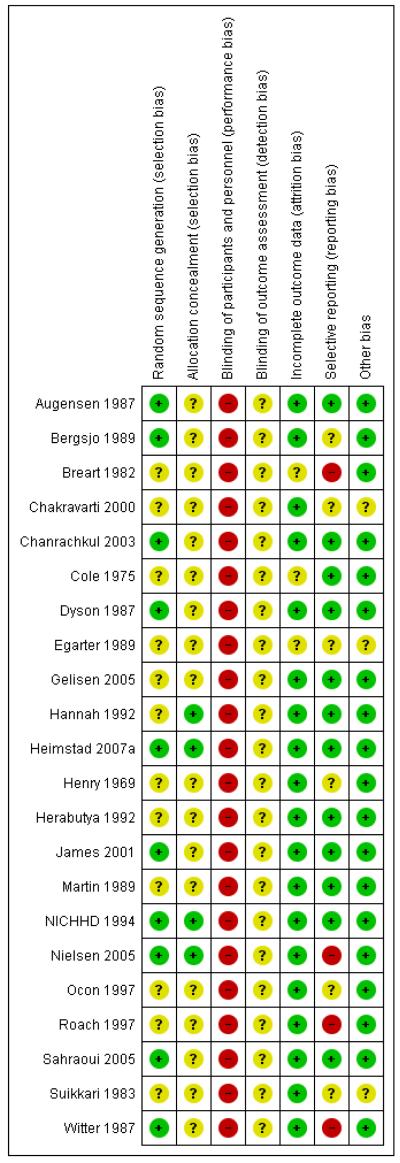
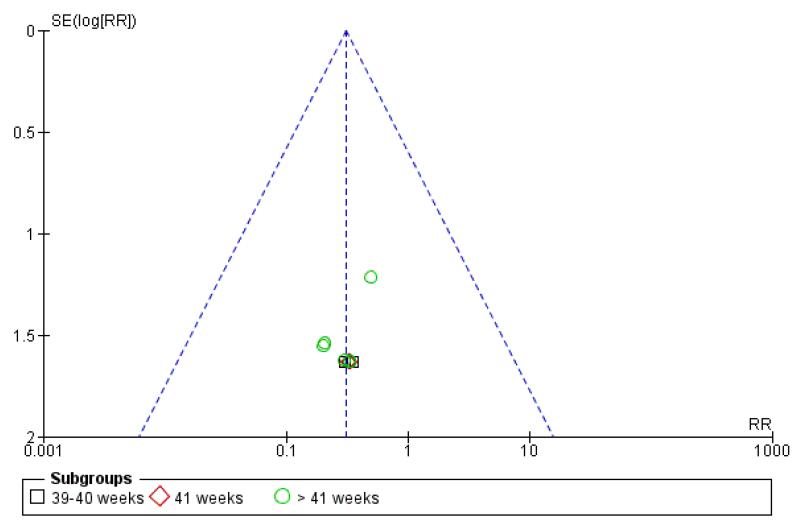
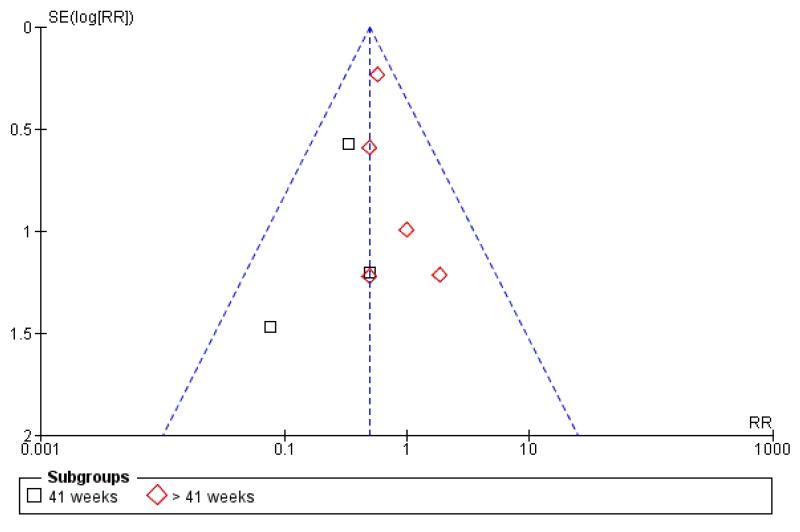
Main results: We included 22 trials reporting on 9383 women. The trials were generally at moderate risk of bias.Compared with a policy of expectant management, a policy of labour induction was associated with fewer (all-cause) perinatal deaths: risk ratio (RR) 0.31, 95% confidence interval (CI) 0.12 to 0.88; 17 trials, 7407 women. There was one perinatal death in the labour induction policy group compared with 13 perinatal deaths in the expectant management group. The number needed to treat to benefit (NNTB) with induction of labour in order to prevent one perinatal death was 410 (95% CI 322 to 1492).For the primary outcome of perinatal death and most other outcomes, no differences between timing of induction subgroups were seen; the majority of trials adopted a policy of induction at 41 completed weeks (287 days) or more.Fewer babies in the labour induction group had meconium aspiration syndrome (RR 0.50, 95% CI 0.34 to 0.73; eight trials, 2371 infants) compared with a policy of expectant management. There was no statistically significant difference between the rates of neonatal intensive care unit (NICU) admission for induction compared with expectant management (RR 0.90, 95% CI 0.78 to 1.04; 10 trials, 6161 infants). For women in the policy of induction arms of trials, there were significantly fewer caesarean sections compared with expectant management in 21 trials of 8749 women (RR 0.89, 95% CI 0.81 to 0.97).
Authors' conclusions: A policy of labour induction compared with expectant management is associated with fewer perinatal deaths and fewer caesarean sections. Some infant morbidities such as meconium aspiration syndrome were also reduced with a policy of post-term labour induction although no significant differences in the rate of NICU admission were seen.However, the absolute risk of perinatal death is small. Women should be appropriately counselled in order to make an informed choice between scheduled induction for a post-term pregnancy or monitoring without induction (or delayed induction).
Figures
Update of
-
Induction of labour for improving birth outcomes for women at or beyond term.Cochrane Database Syst Rev. 2006 Oct 18;(4):CD004945. doi: 10.1002/14651858.CD004945.pub2. Cochrane Database Syst Rev. 2006. Update in: Cochrane Database Syst Rev. 2012 Jun 13;(6):CD004945. doi: 10.1002/14651858.CD004945.pub3. PMID: 17054226 Updated.
References
References to studies included in this review
-
- Augensen K, Bergsjo P, Eikeland T, Askvik K, Carlsen J. Induction of labour in prolonged pregnancy. A prospective randomized study; Proceedings of 10th European Congress of Perinatal Medicine; Leipzig, Germany. 12-16 Aug 1986.
-
- Bergsjo P, Huang GD, Yu SQ, Gao Z, Bakketeig LS. Comparison of induced vs non-induced labor in post-term pregnancy. Acta Obstetricia et Gynecologica Scandinavica. 1989;68:683–7. - PubMed
-
- Breart G, Goujard J, Maillard F, Chavigny C, Rumeau-Rouquette C, Sureau C. Comparison of two obstetrical policies with regard to artificial induction of labour at term. A randomised trial. Journal de Gynecologie, Obstetrique et Biologie de la Reproduction. 1982;11:107–12. - PubMed
-
- Chakravarti S, Goenka B. Conservative policy of induction of labor in uncomplicated postdated pregnancies; XVI FIGO World Congress of Obstetrics & Gynecology; Washington DC, USA. 3-8 Sept 2000; p. 62. Book 3.
References to studies excluded from this review
-
- Alcalay M, Hourvitz A, Reichman B, Luski A, Quint J, Barkai G, et al. Prelabour rupture of membranes at term: early induction of labour vs expectant management. European Journal of Obstetrics & Gynecology and Reproductive Biology. 1996;70:129–33. - PubMed
-
- Amano K, Saito K, Shoda T, Tani A, Yoshihara H, Nishijima M. Elective induction of labour at 39 weeks of gestation: a prospective randomized trial. Journal of Obstetrics and Gynaecology Research. 1999;25:33–7. - PubMed
-
- Ascher-Walsh C, Burke B, Baxi L. Outpatient management of prolonged pregnancy with misoprostol (MP): a randomized, double-blind placebo controlled study, prelim. data. American Journal of Obstetrics and Gynecology. 2000;182(1 Pt 2):S20.
-
- Bell RJ, Permezel M, MacLennan, Hughes C, Healy D, Brennecke S. A randomized, double-blind controlled trial of the safety of vaginal recombinant human relaxin for cervical ripening. Obstetrics & Gynecology. 1993;82:328–33. - PubMed
-
- Berghella V, Mickens R. Stripping of membranes as a safe method to reduce prolonged pregnancies; XIV World Congress of Gynecology and Obstetrics (FIGO); Montreal, Canada.. 26-30 Sept 1994. - PubMed
References to ongoing studies
-
- Rijnders MEB. [accessed 15 February 2007];Costs and effects of amniotomy at home for induction of post term pregnancy (ongoing trial) Current Controlled Trials. www.controlled-trials.com.
Additional references
-
- Alfirevic Z, Weeks A. Oral misoprostol for induction of labour. Cochrane Database of Systematic Reviews. 2006;(2) DOI: 10.1002/14651858.CD001338.pub2. - PubMed
-
- Caughey AB, Sundaram V, Kaimal AJ, Gienger A, Cheng YW, McDonald KM, et al. Systematic review: elective induction of labor versus expectant management of pregnancy. Annals of Internal Medicine. 2009;151:252–63. - PubMed
-
- Dare MR, Middleton P, Crowther CA. Planned early birth versus expectant management (waiting) for prelabour rupture of membranes at term (37 weeks or more) Cochrane Database of Systematic Reviews. 2006;(1) DOI: 10.1002/14651858.CD005302.pub2. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources