

Interventions for tobacco cessation in the dental setting
- PMID: 22696348
- PMCID: PMC3916957
- DOI: 10.1002/14651858.CD005084.pub3
Interventions for tobacco cessation in the dental setting
Update in
-
Interventions for tobacco cessation delivered by dental professionals.Cochrane Database Syst Rev. 2021 Feb 19;2(2):CD005084. doi: 10.1002/14651858.CD005084.pub4. Cochrane Database Syst Rev. 2021. PMID: 33605440 Free PMC article.
Abstract
Background: Tobacco use has significant adverse effects on oral health. Oral health professionals in the dental office or community setting have a unique opportunity to increase tobacco abstinence rates among tobacco users.
Objectives: This review assesses the effectiveness of interventions for tobacco cessation delivered by oral health professionals and offered to cigarette smokers and smokeless tobacco users in the dental office or community setting.
Search methods: We searched the Cochrane Tobacco Addiction Group Specialized Register (CENTRAL), MEDLINE (1966-November 2011), EMBASE (1988-November 2011), CINAHL (1982-November 2011), Healthstar (1975-November 2011), ERIC (1967-November 2011), PsycINFO (1984-November 2011), National Technical Information Service database (NTIS, 1964-November 2011), Dissertation Abstracts Online (1861-November 2011), Database of Abstract of Reviews of Effectiveness (DARE, 1995-November 2011), and Web of Science (1993-November 2011).
Selection criteria: We included randomized and pseudo-randomized clinical trials assessing tobacco cessation interventions conducted by oral health professionals in the dental office or community setting with at least six months of follow-up.
Data collection and analysis: Two authors independently reviewed abstracts for potential inclusion and abstracted data from included trials. Disagreements were resolved by consensus. The primary outcome was abstinence from smoking or all tobacco use (for users of smokeless tobacco) at the longest follow-up, using the strictest definition of abstinence reported. The effect was summarised as an odds ratio, with correction for clustering where appropriate. Heterogeneity was assessed using the I² statistic and where appropriate a pooled effect was estimated using an inverse variance fixed-effect model.
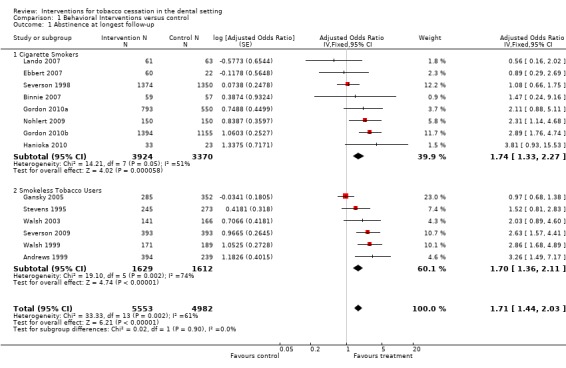
Main results: Fourteen clinical trials met the criteria for inclusion in this review. Included studies assessed the efficacy of interventions in the dental office or in a community school or college setting. Six studies evaluated the effectiveness of interventions among smokeless tobacco (ST) users, and eight studies evaluated interventions among cigarette smokers, six of which involved adult smokers in dental practice settings. All studies employed behavioral interventions and only one required pharmacotherapy as an interventional component. All studies included an oral examination component. Pooling all 14 studies suggested that interventions conducted by oral health professionals can increase tobacco abstinence rates (odds ratio [OR] 1.71, 95% confidence interval [CI] 1.44 to 2.03) at six months or longer, but there was evidence of heterogeneity (I² = 61%). Within the subgroup of interventions for smokers, heterogeneity was smaller (I² = 51%), but was largely attributable to a large study showing no evidence of benefit. Within this subgroup there were five studies which involved adult smokers in dental practice settings. Pooling these showed clear evidence of benefit and minimal heterogeneity (OR 2.38, 95% CI 1.70 to 3.35, 5 studies, I² = 3%) but this was a posthoc subgroup analysis. Amongst the studies in smokeless tobacco users the heterogeneity was also attributable to a large study showing no sign of benefit, possibly due to intervention spillover to control colleges; the other five studies indicated that interventions for ST users were effective (OR 1.70; 95% CI 1.36 to 2.11).
Authors' conclusions: Available evidence suggests that behavioral interventions for tobacco cessation conducted by oral health professionals incorporating an oral examination component in the dental office or community setting may increase tobacco abstinence rates among both cigarette smokers and smokeless tobacco users. Differences between the studies limit the ability to make conclusive recommendations regarding the intervention components that should be incorporated into clinical practice, however, behavioral counselling (typically brief) in conjunction with an oral examination was a consistent intervention component that was also provided in some control groups.
Conflict of interest statement
None.
Figures



Update of
-
Interventions for tobacco cessation in the dental setting.Cochrane Database Syst Rev. 2006 Jan 25;(1):CD005084. doi: 10.1002/14651858.CD005084.pub2. Cochrane Database Syst Rev. 2006. Update in: Cochrane Database Syst Rev. 2012 Jun 13;(6):CD005084. doi: 10.1002/14651858.CD005084.pub3. PMID: 16437517 Updated.
References
References to studies included in this review
-
- Andrews JA, Severson H, Lichtenstein E, Gordon JS, Barckley MF. Evaluation of a dental office tobacco cessation program: effects on smokeless tobacco use. Annals of Behavioral Medicine 1999;21:48‐53. - PubMed
- Gordon JS, Severson HH. Tobacco cessation through dental office settings. Journal of Dental Education 2001;65(4):354‐63. - PubMed
- Severson HH, Andrews JA, Lichtenstein E, Gordon JS, Barckley MF. Using the hygiene visit to deliver a tobacco cessation program: results of a randomized clinical trial. Journal of the American Dental Association 1998;129(7):993‐9. - PubMed
-
- Ebbert JO, Carr AB, Patten CA, Morris RA, Schroeder DR. Tobacco use quitline enrollment through dental practices: a pilot study. Journal of the American Dental Association 2007;138(5):595‐601. - PubMed
-
- Ellison J, Gansky SA, Kavanagh C, Rudy D, et al. An Athletic Trainer‐Mediated Spit Tobacco Prevention and Cessation Program (IADR San Diego 2002 abstracts). Journal of Dental Research 2002;81(March, Special Issue A):A‐494 (Abs 4047).
- Gansky SA, Ellison JA, Rudy D, Bergert N, Letendre MA, Nelson L, et al. Cluster randomized controlled trial of an athletic trainer‐directed spit (smokeless) tobacco intervention for college baseball athletes: results after one year. Journal of Athletic Training 2005;40(2):76‐87. - PMC - PubMed
References to studies excluded from this review
-
- Albert DA, Anluwalia KP, Ward A, Sadowsky D. The use of 'academic detailing' to promote tobacco‐use cessation counseling in dental offices. Journal of the American Dental Association 2004;135(12):1700‐6. - PubMed
-
- Barker GJ, Taylor TS, Barker BF. Implementation of a tobacco cessation program in the student clinics. Journal of Dental Education 1995;59(8):850‐5. - PubMed
-
- Barker GJ, Williams KB, Taylor TS, Barker BF. Practice behaviors of alumni trained as students in tobacco use cessation interventions. Journal of Dental Hygiene 2001;75(2):165‐9. - PubMed
-
- Binnie V, McHugh S, MacPherson LM, Jenkins W, et al. Dental hygienists' delivery of smoking cessation: 3‐month outcomes (JDR Abstract). Journal of Dental Research 2003;82(Special Issue B, June):B‐373.
Additional references
-
- Bandura A. Social foundations of thought and action: a social cognitive theory. New Jersey: Prentice‐Hall, Inc., 1986.
-
- Block DE, Block LE, Hutton SJ, Johnson KM. Tobacco counseling practices of dentists compared to other health care providers in a midwestern region. Journal of Dental Education 1999;63(11):821‐7. - PubMed
-
- Bowles WH, Wilkinson MR, Wagner MJ, Woody RD. Abrasive particles in tobacco products: a possible factor in dental attrition. Journal of the American Dental Association 1995;126(3):327‐31. - PubMed
-
- Campbell HS, Macdonald JM. Tobacco counselling among Alberta dentists. Journal of the Canadian Dental Association1994; Vol. 60, issue 3:218‐20, 223‐6. - PubMed
-
- Campbell HS, Sletten M, Petty T. Patient perceptions of tobacco cessation services in dental offices. Journal of the American Dental Association 1999;130(2):219‐26. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous