Hospitalizations for respiratory syncytial virus bronchiolitis in preterm infants at <33 weeks gestation without bronchopulmonary dysplasia: the CASTOR study
- PMID: 22697130
- PMCID: PMC3594836
- DOI: 10.1017/S0950268812001069
Hospitalizations for respiratory syncytial virus bronchiolitis in preterm infants at <33 weeks gestation without bronchopulmonary dysplasia: the CASTOR study
Abstract
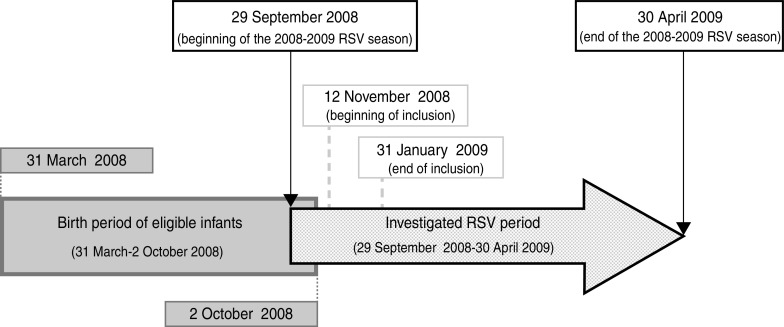
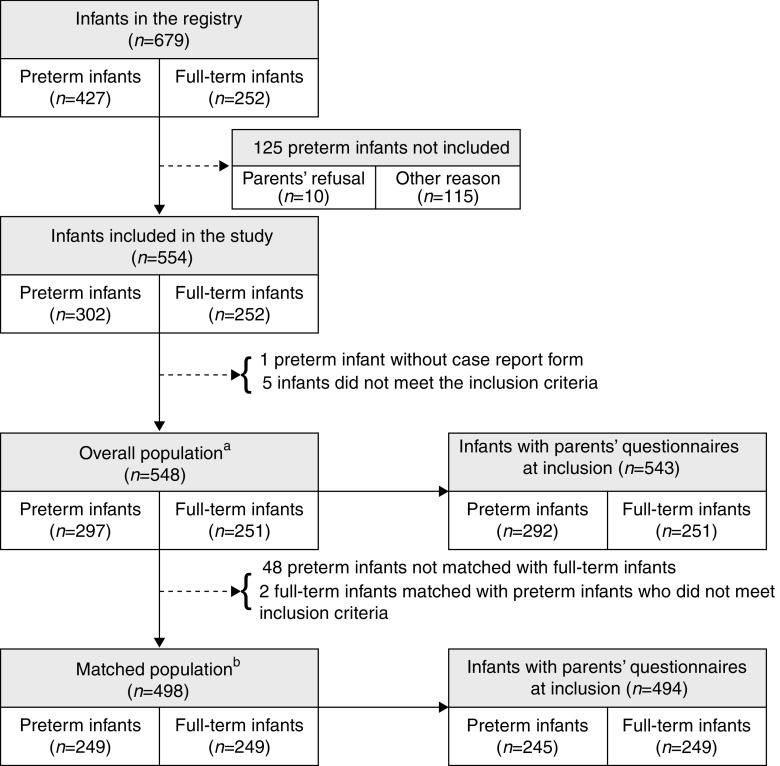
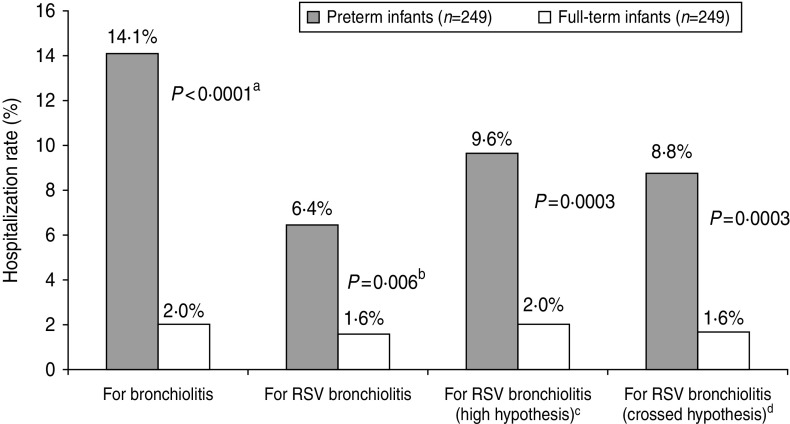
This study was conducted during the 2008-2009 respiratory syncytial virus (RSV) season in France to compare hospitalization rates for bronchiolitis (RSV-confirmed and all types) between very preterm infants (<33 weeks' gestational age, WGA) without bronchopulmonary dysplasia and full-term infants (39-41 WGA) matched for date of birth, gender and birth location, and to evaluate the country-specific risk factors for bronchiolitis hospitalization. Data on hospitalizations were collected both retrospectively and prospectively for 498 matched infants (249 per group) aged <6 months at the beginning of the RSV season. Compared to full-term infants, preterm infants had a fourfold [95% confidence interval (CI) 1·36-11·80] and a sevenfold (95% CI 2·79-17·57) higher risk of being hospitalized for bronchiolitis, RSV-confirmed and all types, respectively. Prematurity was the only factor that significantly increased the risk of being hospitalized for bronchiolitis. The risk of multiple hospitalizations for bronchiolitis in the same infant significantly increased with male gender and the presence of siblings aged ⩾2 years.
Figures
References
-
- Grimprel E. Epidemiology of infant bronchiolitis in France. Archives de Pédiatrie 2001; 8: 83–92. - PubMed
-
- Shay DK, et al. Bronchiolitis-associated mortality and estimates of respiratory syncytial virus-associated deaths among US Children, 1979–1997. Journal of Infectious Diseases 2001; 183: 16–22. - PubMed
-
- Agence Nationale d'Accréditation et d'Evaluation en Santé (ANAES). Consensus conference. Management of bronchiolitis in infants. 2000. (http://www.has-sante.fr/portail/upload/docs/application/pdf/Bronchioliti...). Accessed 23 March 2012.
-
- Busch A, Thomson AH. Acute bronchiolitis. British Medical Journal. Published online: 17 November 2007. doi: 10.1136/bmj.39374.600081.AD. - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical