

Prediction of pathological and oncological outcomes based on extended prostate biopsy results in patients with prostate cancer receiving radical prostatectomy: a single institution study
- PMID: 22697234
- PMCID: PMC3449198
- DOI: 10.1186/1746-1596-7-68
Prediction of pathological and oncological outcomes based on extended prostate biopsy results in patients with prostate cancer receiving radical prostatectomy: a single institution study
Abstract
Background: The prediction of pathological outcomes prior to surgery remains a challenging problem for the appropriate surgical indication of prostate cancer. This study was performed to identify preoperative values predictive of pathological and oncological outcomes based on standardized extended prostate biopsies with core histological results diagrammed/mapped in patients receiving radical prostatectomy for prostate cancer clinically diagnosed as localized or locally advanced disease.
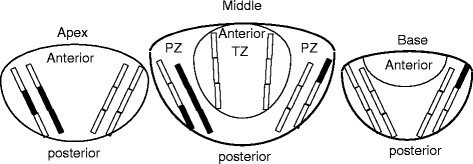
Methods: In 124 patients with clinically localized or locally advanced prostate cancer (cT1c-cT3a) without prior treatment, pathological outcomes on the surgical specimen including seminal vesicle involvement (SVI), positive surgical margin (PSM), and perineural invasion (PNI) were studied in comparison with clinical parameters based on the results of 14-core prostate biopsies comprising sextant, laterally-directed sextant, and bilateral transition zone (TZ) sampling.
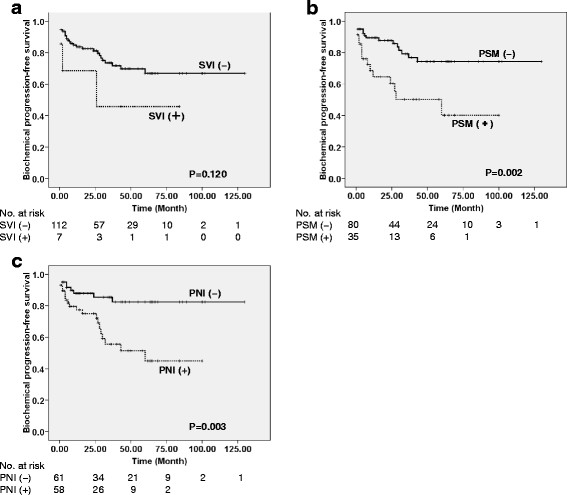
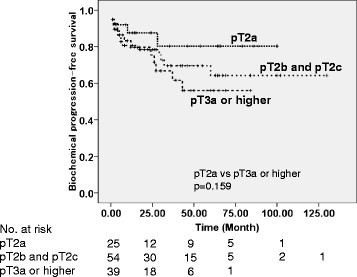
Results: Concerning the association of pathological outcomes with oncological outcomes, patients with PSM and PNI on surgical specimens had poorer biochemical-progression-free survival than those without PSM (logrank p = 0.002) and PNI (p = 0.003); it was also poorer concerning SVI, although the difference was not significant (p = 0.120). Concerning the impact of clinical parameters on these pathological outcomes, positive TZ and multiple positive biopsy cores in the prostatic middle were independent values predictive of SVI with multivariate analyses (p = 0.020 and p = 0.025, respectively); both positive TZ and multiple positive prostatic middle biopsies were associated with larger tumor volume (p < 0.001 in both). The percentage of positive biopsy cores (%positive cores) and biopsy Gleason score were independent values predictive of PSM (p = 0.001) and PNI (p = 0.001), respectively. Multiple positive cores in the prostatic base were associated with proximal/bladder-side PSM (p < 0.001), and also linked to poorer biochemical-progression-free survival (p = 0.004). Clinical T stage had no association with these pathological outcomes.
Conclusions: %positive cores and Gleason score in extended biopsies were independent values predictive of PSM and PNI in prostate cancer clinically diagnosed as localized or locally advanced disease, respectively, which were associated with poorer oncological outcomes. When diagramming biopsy-core results, extended biopsy may provide additional information for predicting oncological and pathological outcomes including SVI in patients clinically diagnosed as having localized or locally advanced disease.
Virtual slides: The virtual slide(s) for this article can be found here: http://www.diagnosticpathology.diagnomx.eu/vs/8790262771042628.
Figures
References
-
- Partin AW, Kattan MW, Subong EN, Walsh PC, Wojno KJ, Oesterling JE, Scardino PT, Pearson JD. Combination of prostate-specific antigen, clinical stage, and Gleason score to predict pathological stage of localized prostate cancer: a multi-institutional update. JAMA. 1997;277:1445–1451. doi: 10.1001/jama.1997.03540420041027. - DOI - PubMed
-
- Swanson GP, Goldman B, Tangen CM, Chin J, Messing E, Canby-Hagino E, Forman JD, Thompson IM, Crawford ED. The prognostic impact of seminal vesicle involvement found at prostatectomy and the effects of adjuvant radiation: data from Southwest Oncology Group 8794. J Urol. 2008;180:2453–2458. doi: 10.1016/j.juro.2008.08.037. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
