

Cost evaluation of cardiovascular magnetic resonance versus coronary angiography for the diagnostic work-up of coronary artery disease: application of the European Cardiovascular Magnetic Resonance registry data to the German, United Kingdom, Swiss, and United States health care systems
- PMID: 22697303
- PMCID: PMC3461475
- DOI: 10.1186/1532-429X-14-35
Cost evaluation of cardiovascular magnetic resonance versus coronary angiography for the diagnostic work-up of coronary artery disease: application of the European Cardiovascular Magnetic Resonance registry data to the German, United Kingdom, Swiss, and United States health care systems
Abstract
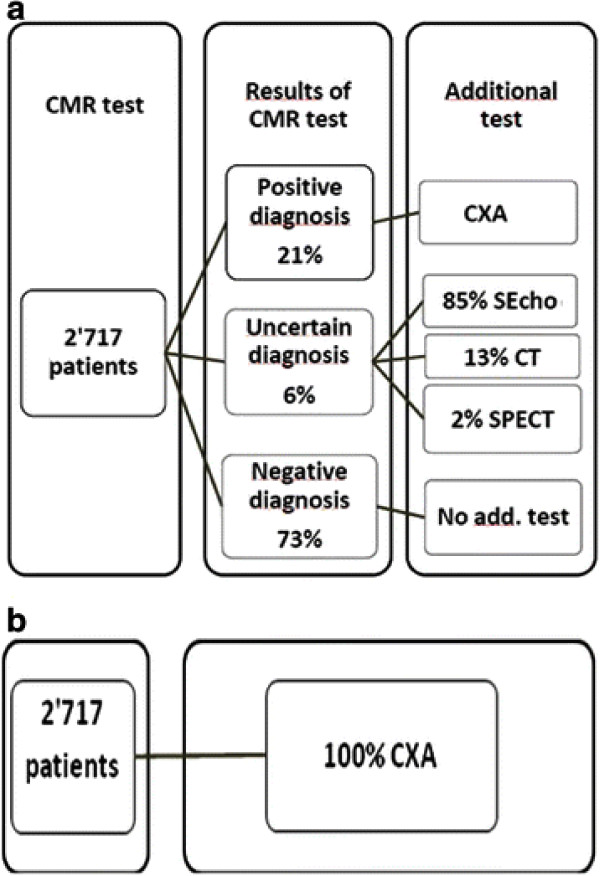
Background: Cardiovascular magnetic resonance (CMR) has favorable characteristics for diagnostic evaluation and risk stratification of patients with known or suspected CAD. CMR utilization in CAD detection is growing fast. However, data on its cost-effectiveness are scarce. The goal of this study is to compare the costs of two strategies for detection of significant coronary artery stenoses in patients with suspected coronary artery disease (CAD): 1) Performing CMR first to assess myocardial ischemia and/or infarct scar before referring positive patients (defined as presence of ischemia and/or infarct scar to coronary angiography (CXA) versus 2) a hypothetical CXA performed in all patients as a single test to detect CAD.
Methods: A subgroup of the European CMR pilot registry was used including 2,717 consecutive patients who underwent stress-CMR. From these patients, 21% were positive for CAD (ischemia and/or infarct scar), 73% negative, and 6% uncertain and underwent additional testing. The diagnostic costs were evaluated using invoicing costs of each test performed. Costs analysis was performed from a health care payer perspective in German, United Kingdom, Swiss, and United States health care settings.
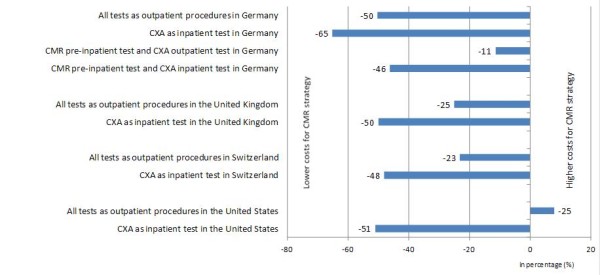
Results: In the public sectors of the German, United Kingdom, and Swiss health care systems, cost savings from the CMR-driven strategy were 50%, 25% and 23%, respectively, versus outpatient CXA. If CXA was carried out as an inpatient procedure, cost savings were 46%, 50% and 48%, respectively. In the United States context, cost savings were 51% when compared with inpatient CXA, but higher for CMR by 8% versus outpatient CXA.
Conclusion: This analysis suggests that from an economic perspective, the use of CMR should be encouraged as a management option for patients with suspected CAD.
Figures
References
-
- Scarborough P, Bhatnagar P, Wickramasinghe K, Smolina K, Mitchell C, Rayner M. Coronary Heart Disease Statistics. 2010. British Heart Foundation; 2010.
-
- WHO. The Atlas of Heart Disease and Stroke. World Health Organization; 2004.
-
- Rosamond W, Flegal K, Furie K. et al. Heart Disease and Stroke Statistics—2008 Update: A Report From the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Am Heart Soc Circ. 2008;117:e25–e26. - PubMed
-
- Schweizerische Eidgenossenschaft. Décès: nombre, évolution et causes 2004 and 2008. Office fédéral de la statistique; 2009.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
