

Comparison of exercise electrocardiography and stress perfusion CMR for the detection of coronary artery disease in women
- PMID: 22697372
- PMCID: PMC3411505
- DOI: 10.1186/1532-429X-14-36
Comparison of exercise electrocardiography and stress perfusion CMR for the detection of coronary artery disease in women
Abstract
Background: Exercise electrocardiography (ECG) is frequently used in the work-up of patients with suspected coronary artery disease (CAD), however the accuracy is reduced in women. Cardiovascular magnetic resonance (CMR) stress testing can accurately diagnose CAD in women. To date, a direct comparison of CMR to ECG has not been performed.
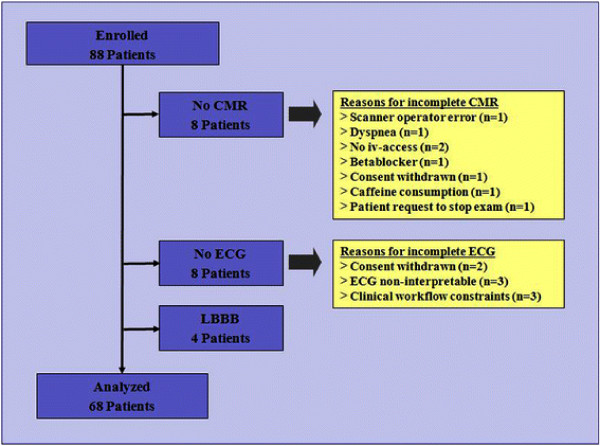
Methods and results: We prospectively enrolled 88 consecutive women with chest pain or other symptoms suggestive of CAD. Patients underwent a comprehensive clinical evaluation, exercise ECG, a CMR stress test including perfusion and infarct imaging, and x-ray coronary angiography (CA) within 24 hours. CAD was defined as stenosis ≥70% on quantitative analysis of CA.Exercise ECG, CMR and CA was completed in 68 females (age 66.4 ± 8.8 years, number of CAD risk factors 3.5±1.4). The prevalence of CAD on CA was 29%. The Duke treadmill score (DTS) in the entire group was -3.0±5.4 and was similar in those with and without CAD (-4.5±5.8 and -2.4±5.1; P=0.12). Sensitivity, specificity and accuracy for CAD diagnosis was higher for CMR compared with exercise ECG (sensitivities 85% and 50%, P=0.02, specificities 94% and 73%, P=0.01, and accuracies 91% and 66%, P=0.0007, respectively). Even after applying the DTS the accuracy of CMR was higher compared to exercise ECG (area under ROC curve 0.94±0.03 vs 0.56±0.07; P=0.0001).
Conclusions: In women with intermediate-to-high risk for CAD who are able to exercise and have interpretable resting ECG, CMR stress perfusion imaging has higher accuracy for the detection of relevant obstruction of the epicardial coronaries when directly compared to exercise ECG.
Figures


References
-
- American heart association. Heart disease and stroke statistics - 2010 update. American heart association, Dallas, Texas; 2010.
-
- Gibbons RJ, Abrams J, Chatterjee K, Daley J, Deedwania PC, Douglas JS, Ferguson TB, Fihn SD, Fraker TD, Gardin JM, O’Rourke RA, Pasternak RC, Williams SV, Alpert JS, Antman EM, Hiratzka LF, Fuster V, Faxon DP, Gregoratos G, Jacobs AK, Smith SC. ACC/AHA 2002 guideline update for the management of patients with chronic stable angina–summary article: A report of the american college of cardiology/american heart association task force on practice guidelines (committee on the management of patients with chronic stable angina) Circulation. 2003;107:148–149.
-
- Grady DCL, Kristof M. Results of systematic review of research on diagnosis and treatment of coronary heart disease in women. Evidence report/technology assessment no. 80. (prepared by the university of california, san francisco-stanford evidence-based practice center under contract no 290-97-0013. ahrq publication no. 03–0035, Rockville, md; 2003.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
