

Aortic valve calcium independently predicts coronary and cardiovascular events in a primary prevention population
- PMID: 22698532
- PMCID: PMC3376353
- DOI: 10.1016/j.jcmg.2011.12.023
Aortic valve calcium independently predicts coronary and cardiovascular events in a primary prevention population
Erratum in
- JACC Cardiovasc Imaging. 2012 Aug;5(8):859
Abstract
Objectives: This study sought to test whether aortic valve calcium (AVC) is independently associated with coronary and cardiovascular events in a primary-prevention population.
Background: Aortic sclerosis is associated with increased cardiovascular morbidity and mortality among the elderly, but the mechanisms underlying this association remain controversial. Also, it is unknown whether this association extends to younger individuals.
Methods: We performed a prospective analysis of 6,685 participants in MESA (Multi-Ethnic Study of Atherosclerosis). All subjects, ages 45 to 84 years and free of clinical cardiovascular disease at baseline, underwent computed tomography for AVC and coronary artery calcium scoring. The primary, pre-specified combined endpoint of cardiovascular events included myocardial infarctions, fatal and nonfatal strokes, resuscitated cardiac arrest, and cardiovascular death, whereas a secondary combined endpoint of coronary events excluded strokes. The association between AVC and clinical events was assessed using Cox proportional hazards regression with incremental adjustments for demographics, cardiovascular risk factors, inflammatory biomarkers, and subclinical coronary atherosclerosis.
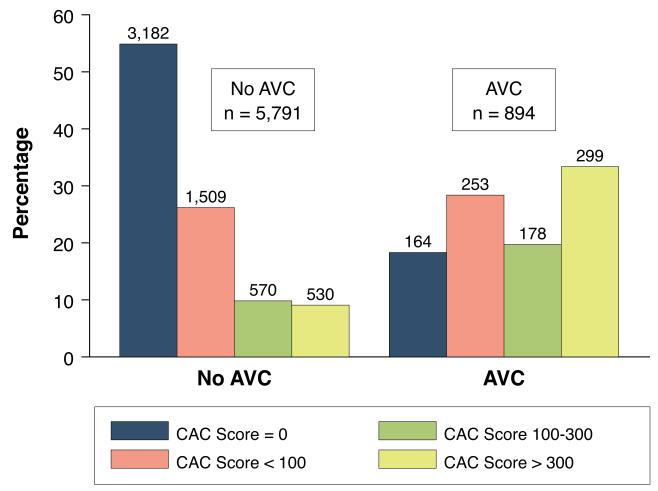
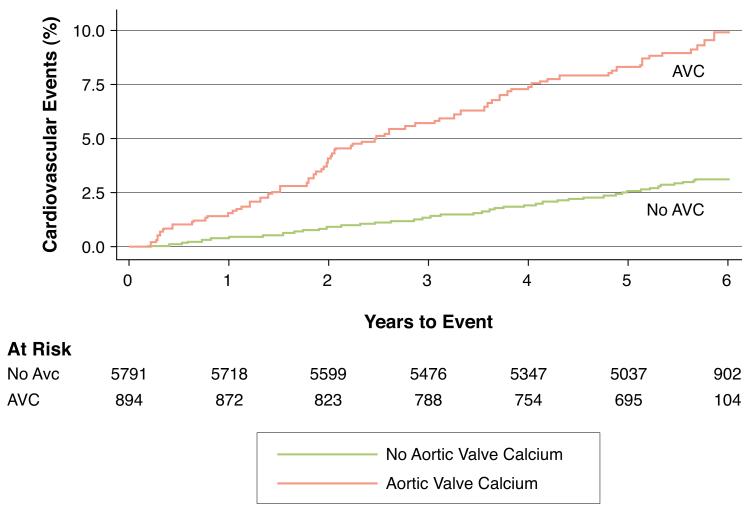
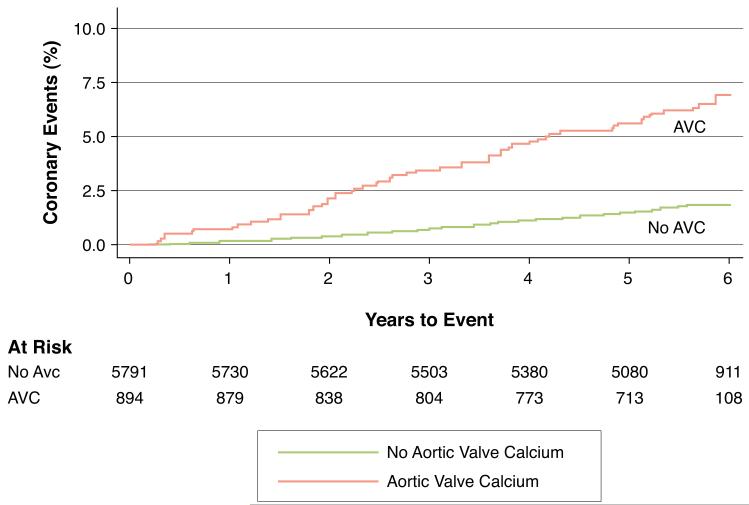
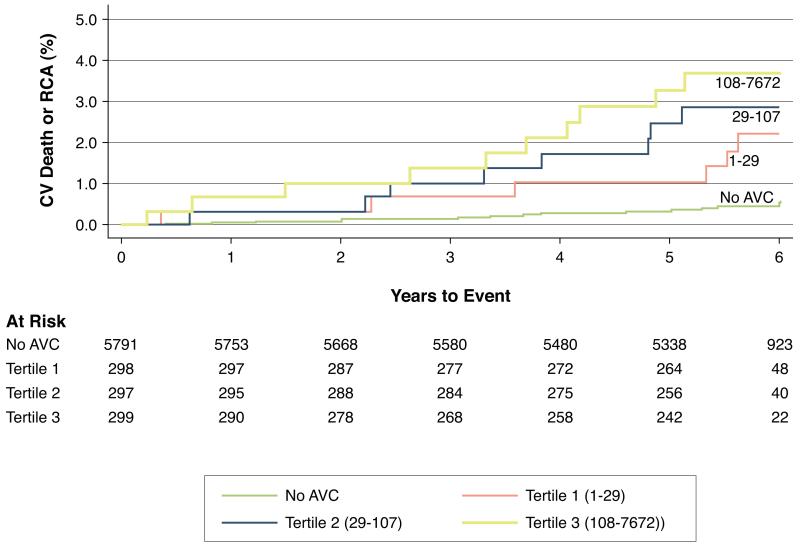
Results: Over a median follow-up of 5.8 years (interquartile range: 5.6 to 5.9 years), adjusting for demographics and cardiovascular risk factors, subjects with AVC (n = 894, 13.4%) had higher risks of cardiovascular (hazard ratio [HR]: 1.50; 95% confidence interval [CI]: 1.10 to 2.03) and coronary (HR: 1.72; 95% CI: 1.19 to 2.49) events compared with those without AVC. Adjustments for inflammatory biomarkers did not alter these associations, but adjustment for coronary artery calcium substantially attenuated both cardiovascular (HR: 1.32; 95% CI: 0.98 to 1.78) and coronary (HR: 1.41; 95% CI: 0.98 to 2.02) event risk. AVC remained predictive of cardiovascular mortality even after full adjustment (HR: 2.51; 95% CI: 1.22 to 5.21).
Conclusions: In this MESA cohort, free of clinical cardiovascular disease, AVC predicts cardiovascular and coronary event risk independent of traditional risk factors and inflammatory biomarkers, likely due to the strong correlation between AVC and subclinical atherosclerosis. The association of AVC with excess cardiovascular mortality beyond coronary atherosclerosis risk merits further investigation. (Multi-Ethnic Study of Atherosclerosis [MESA]; NCT00005487).
Copyright © 2012 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Stewart BF, Siscovick D, Lind BK, et al. Clinical factors associated with calcific aortic valve disease. Cardiovascular Health Study. J Am Coll Cardiol. 1997;29:630–4. - PubMed
-
- Agmon Y, Khandheria BK, Meissner I, et al. Aortic valve sclerosis and aortic atherosclerosis: different manifestations of the same disease? Insights from a population-based study. J Am Coll Cardiol. 2001;38:827–34. - PubMed
-
- Lindroos M, Kupari M, Valvanne J, Strandberg T, Heikkila J, Tilvis R. Factors associated with calcific aortic valve degeneration in the elderly. Eur Heart J. 1994;15:865–70. - PubMed
-
- O’Brien KD. Pathogenesis of Calcific Aortic Valve Disease. A Disease Process Comes of Age (and a Good Deal More) Arterioscler Thromb Vasc Biol. 2006 - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
- R01 HL071739/HL/NHLBI NIH HHS/United States
- N01 HC095169/HL/NHLBI NIH HHS/United States
- N01 HC095161/HC/NHLBI NIH HHS/United States
- N01 HC095164/HC/NHLBI NIH HHS/United States
- N01-HC-95159/HC/NHLBI NIH HHS/United States
- N01 HC095159/HL/NHLBI NIH HHS/United States
- R01 HL063963/HL/NHLBI NIH HHS/United States
- R01-HL-63963-01A1/HL/NHLBI NIH HHS/United States
- N01-HC-95169/HC/NHLBI NIH HHS/United States
- N01 HC095169/HC/NHLBI NIH HHS/United States
- N01 HC095165/HC/NHLBI NIH HHS/United States
- KL2 TR002317/TR/NCATS NIH HHS/United States
- N01 HC095163/HC/NHLBI NIH HHS/United States
- N01 HC095162/HC/NHLBI NIH HHS/United States
- N01-HC-95165/HC/NHLBI NIH HHS/United States
- N01 HC095160/HC/NHLBI NIH HHS/United States
- N01 HC095159/HC/NHLBI NIH HHS/United States
- HL071739/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
