

Hypoxia-inducible factor 1 transcriptional activity in endothelial cells is required for acute phase cardioprotection induced by ischemic preconditioning
- PMID: 22699503
- PMCID: PMC3387090
- DOI: 10.1073/pnas.1208314109
Hypoxia-inducible factor 1 transcriptional activity in endothelial cells is required for acute phase cardioprotection induced by ischemic preconditioning
Abstract
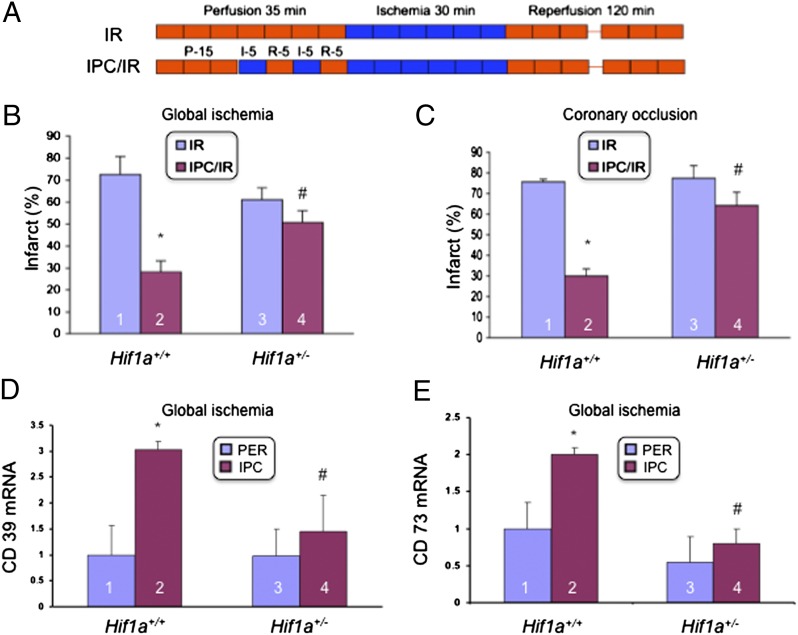
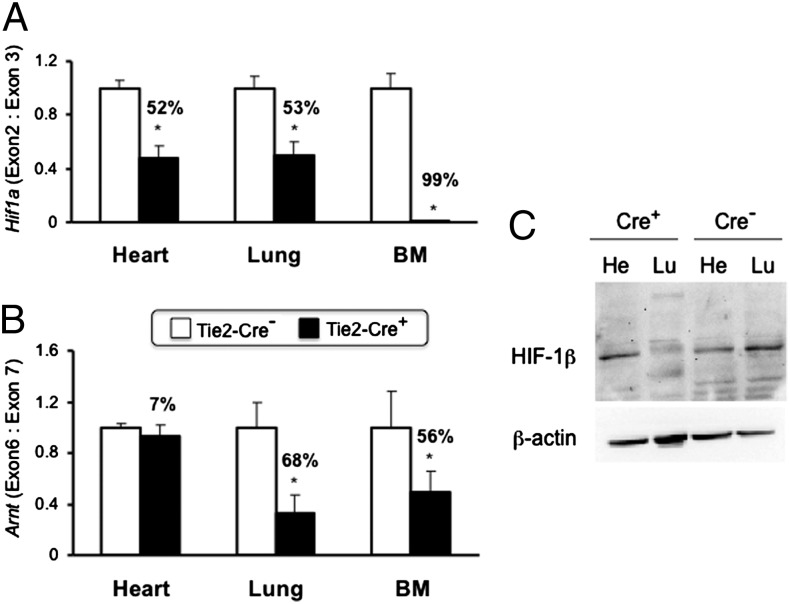
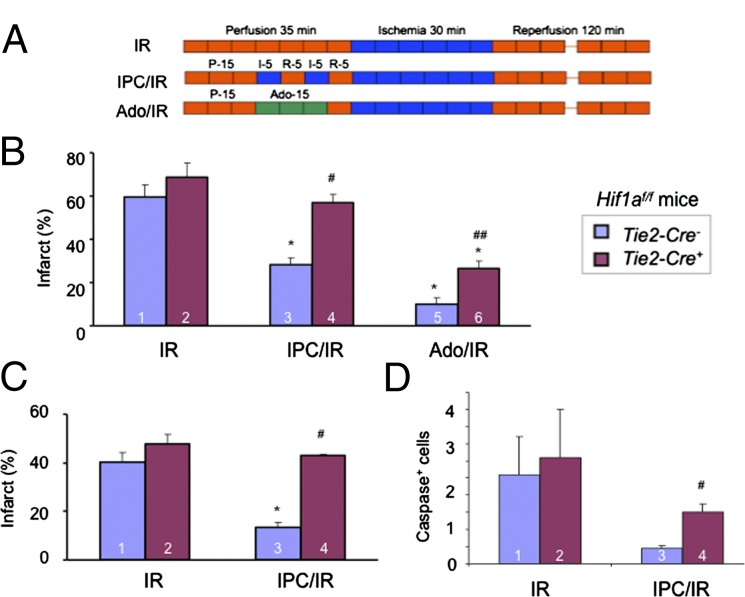
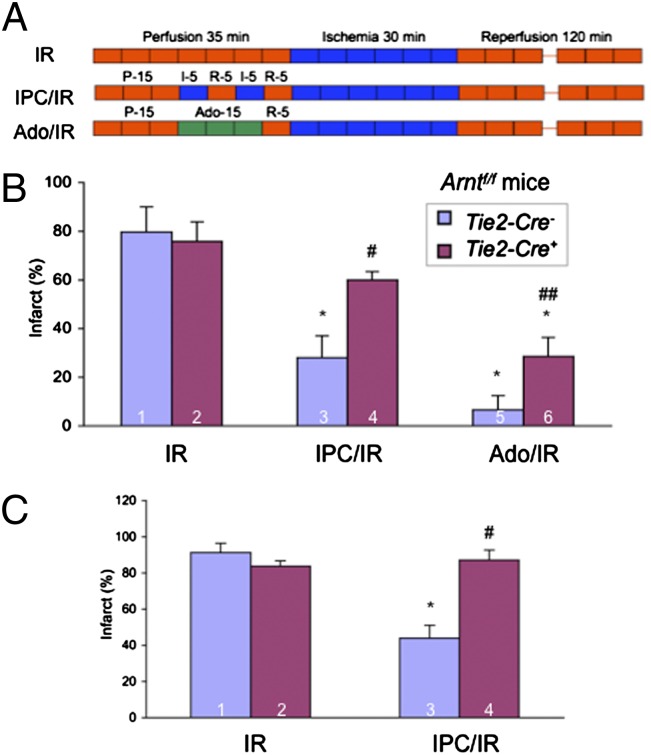
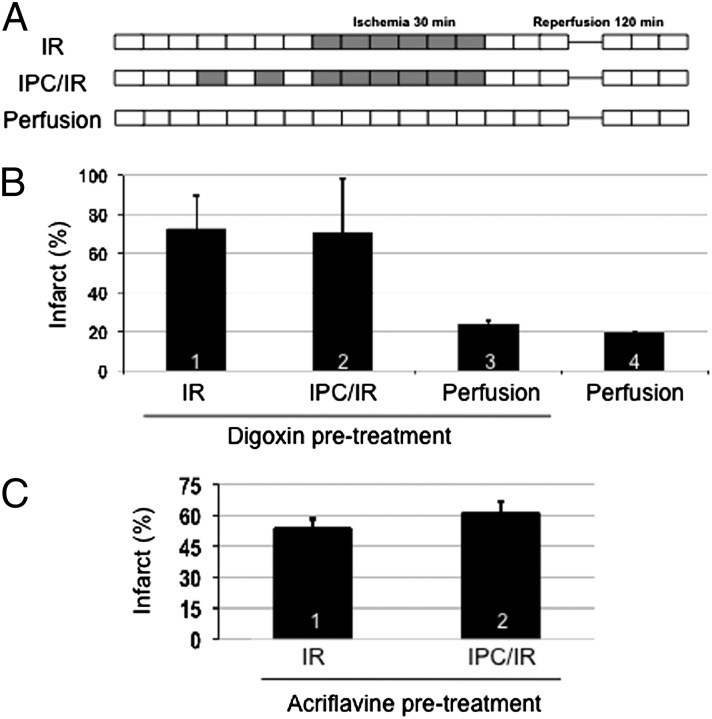
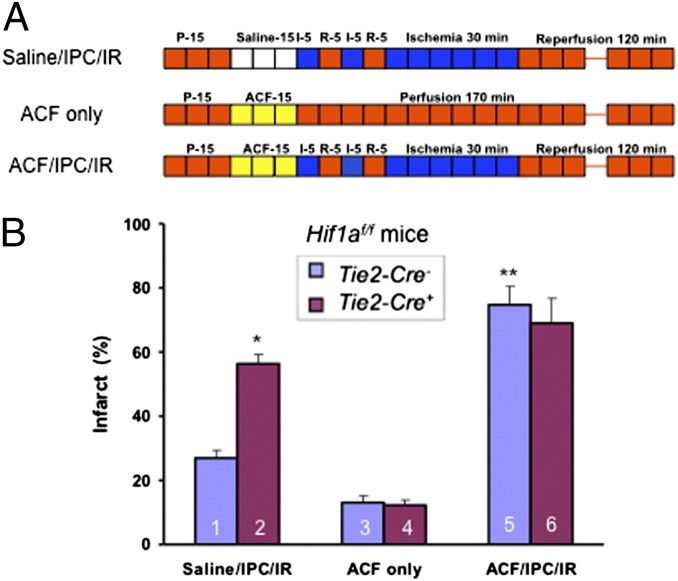
Infarction occurs when myocardial perfusion is interrupted for prolonged periods of time. Short episodes of ischemia and reperfusion protect against tissue injury when the heart is subjected to a subsequent prolonged ischemic episode, a phenomenon known as ischemic preconditioning (IPC). Hypoxia-inducible factor 1 (HIF-1) is a transcription factor that mediates adaptive responses to hypoxia/ischemia and is required for IPC. In this study, we performed a cellular and molecular characterization of the role of HIF-1 in IPC. We analyzed mice with knockout of HIF-1α or HIF-1β in Tie2(+) lineage cells, which include bone marrow (BM) and vascular endothelial cells, compared with control littermates. Hearts were subjected to 30 min of ischemia and 120 min of reperfusion, either as ex vivo Langendorff preparations or by in situ occlusion of the left anterior descending artery. The IPC stimulus consisted of two cycles of 5-min ischemia and 5-min reperfusion. Mice lacking HIF-1α or HIF-1β in Tie2(+) lineage cells showed complete absence of protection induced by IPC, whereas significant protection was induced by adenosine infusion. Treatment of mice with a HIF-1 inhibitor (digoxin or acriflavine) 4 h before Langendorff perfusion resulted in loss of IPC, as did administration of acriflavine directly into the perfusate immediately before IPC. We conclude that HIF-1 activity in endothelial cells is required for acute IPC. Expression and dimerization of the HIF-1α and HIF-1β subunits is required, suggesting that the heterodimer is functioning as a transcriptional activator, despite the acute nature of the response.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Lopaschuk GD, Kelly DP. Signalling in cardiac metabolism. Cardiovasc Res. 2008;79:205–207. - PubMed
-
- Nallamothu BK, Bradley EH, Krumholz HM. Time to treatment in primary percutaneous coronary intervention. N Engl J Med. 2007;357:1631–1638. - PubMed
-
- Murry CE, Jennings RB, Reimer KA. Preconditioning with ischemia: A delay of lethal cell injury in ischemic myocardium. Circulation. 1986;74:1124–1136. - PubMed
-
- Kuzuya T, et al. Delayed effects of sublethal ischemia on the acquisition of tolerance to ischemia. Circ Res. 1993;72:1293–1299. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
Miscellaneous
