

Preference for colonoscopy versus computerized tomographic colonography: a systematic review and meta-analysis of observational studies
- PMID: 22700393
- PMCID: PMC3445696
- DOI: 10.1007/s11606-012-2115-4
Preference for colonoscopy versus computerized tomographic colonography: a systematic review and meta-analysis of observational studies
Abstract
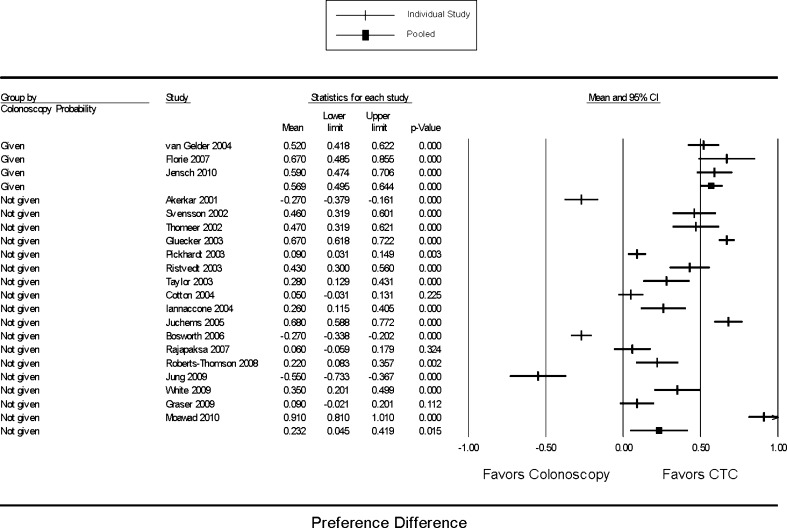
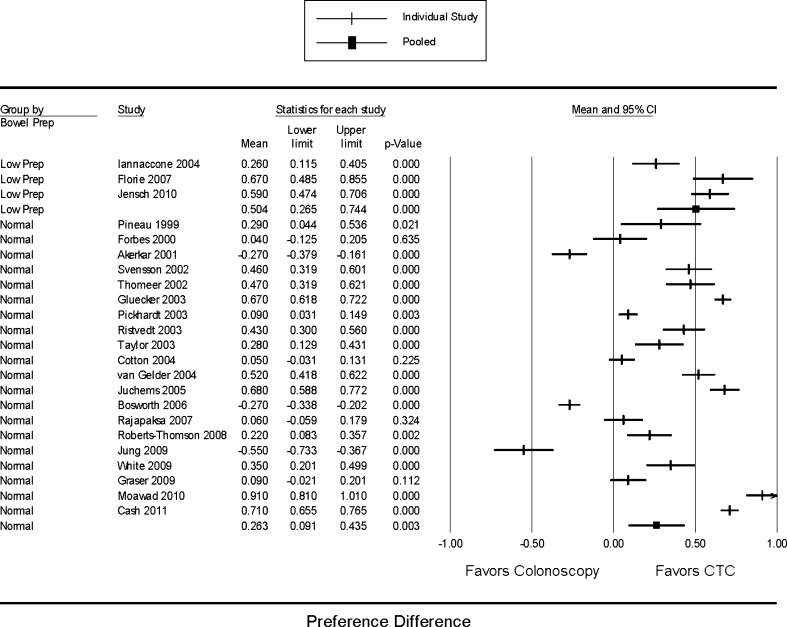
In recent years, colorectal cancer (CRC) screening using computerized tomographic colonography (CTC) has attracted considerable attention. In order to better understand patient preferences for CTC versus colonoscopy, we performed a systematic review and meta-analysis of the available literature. Data sources included published studies, abstracts and book chapters, in any language, with publication dates from 1995 through February 2012, and with prospective or retrospective enrollment of diagnostic or screening patients who had undergone both procedures and explicit assessment of their preference for colonoscopy versus CTC. A predefined algorithm identified eligible studies using computer and hand searches performed by two independent investigators. We used a mixed effects model to pool preference differences (defined as the proportion of subjects who preferred CTC minus the proportion who preferred colonoscopy for each study). Twenty-three studies met inclusion criteria, totaling 5616 subjects. In 16 of these studies, patients preferred CTC over colonoscopy, while colonoscopy was preferred in three studies. Due to the high degree of heterogeneity, an overall pooled preference difference was not calculated. Stratified analysis revealed that studies published in radiology journals (preference difference 0.590 [95 % CI 0.485, 0.694]) seemed more likely than studies in gastroenterology (0.218 [-0.015-0.451]) or general medicine journals (-0.158 [-0.389-0.072]) to report preference for CTC (p<0.001). Studies by radiology authors showed a trend towards stronger preference for CTC compared with studies by gastroenterology authors. Symptomatic patients expressed no preference, but screening patients preferred CTC. There was no difference in preferences between studies using "masked" and "unmasked" preference ascertainment methods. Three studies featuring limited bowel preparations for CTC reported marked preference for CTC. There was no evidence of publication bias, while cumulative and exclusion analysis did not show any temporal trend or dominant study. Limitations included data heterogeneity and preference ascertainment limitations. In conclusion, most included studies reported preference for CTC. On stratified analysis, screening patients preferred CTC while diagnostic patients showed no preference. Studies published in radiology journals showed significantly stronger preference for CTC compared with studies in gastroenterology or general medicine journals.
Figures




References
-
- Levin B, Lieberman DA, McFarland B, et al. Screening and surveillance for the early detection of colorectal cancer and adenomatous polyps, 2008: a joint guideline from the American Cancer Society, the US Multi-Society Task Force on Colorectal Cancer, and the American College of Radiology. Gastroenterology. 2008;134(5):1570–1595. doi: 10.1053/j.gastro.2008.02.002. - DOI - PubMed
-
- Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med. 2009;151(4):264–269. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
