

Kinematic, muscular, and metabolic responses during exoskeletal-, elliptical-, or therapist-assisted stepping in people with incomplete spinal cord injury
- PMID: 22700537
- PMCID: PMC3925942
- DOI: 10.2522/ptj.20110310
Kinematic, muscular, and metabolic responses during exoskeletal-, elliptical-, or therapist-assisted stepping in people with incomplete spinal cord injury
Abstract
Background: Robotic-assisted locomotor training has demonstrated some efficacy in individuals with neurological injury and is slowly gaining clinical acceptance. Both exoskeletal devices, which control individual joint movements, and elliptical devices, which control endpoint trajectories, have been utilized with specific patient populations and are available commercially. No studies have directly compared training efficacy or patient performance during stepping between devices.
Objective: The purpose of this study was to evaluate kinematic, electromyographic (EMG), and metabolic responses during elliptical- and exoskeletal-assisted stepping in individuals with incomplete spinal cord injury (SCI) compared with therapist-assisted stepping. Design A prospective, cross-sectional, repeated-measures design was used.
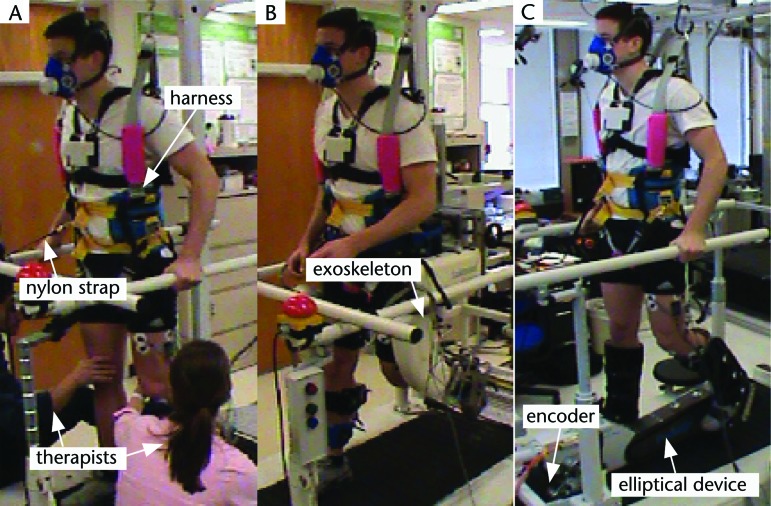
Methods: Participants with incomplete SCI (n=11) performed 3 separate bouts of exoskeletal-, elliptical-, or therapist-assisted stepping. Unilateral hip and knee sagittal-plane kinematics, lower-limb EMG recordings, and oxygen consumption were compared across stepping conditions and with control participants (n=10) during treadmill stepping.
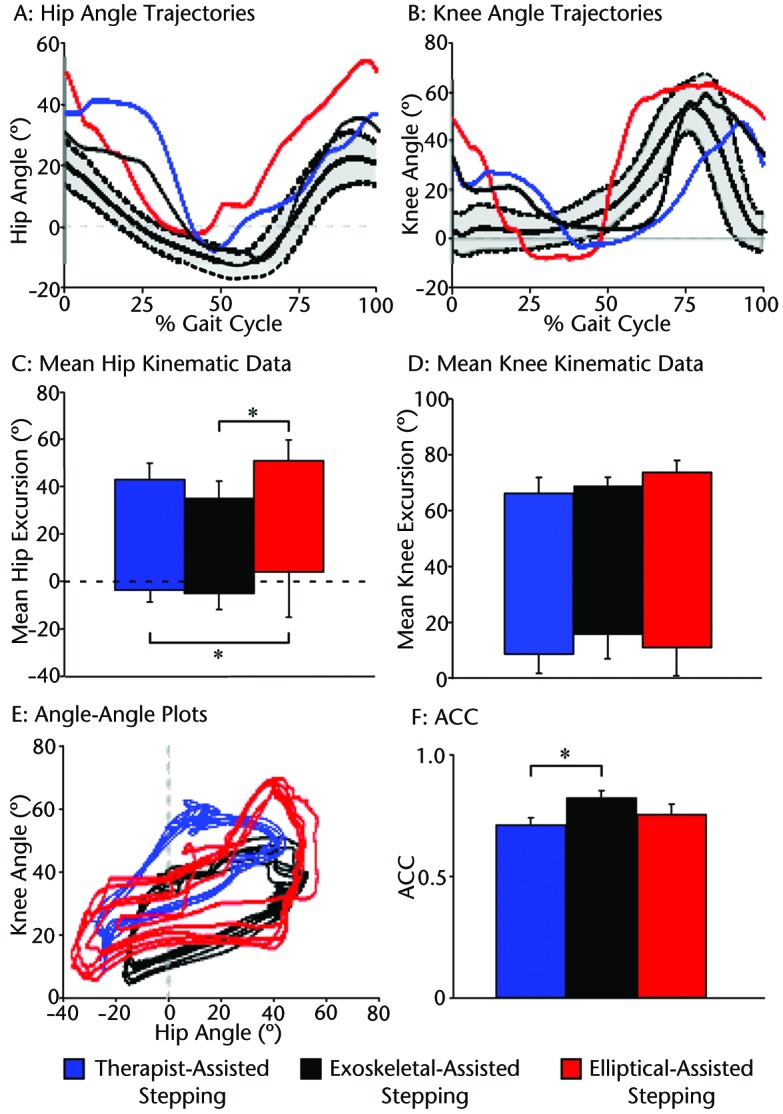
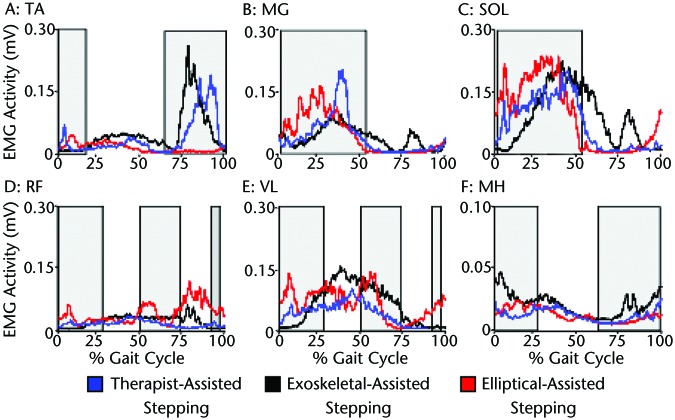
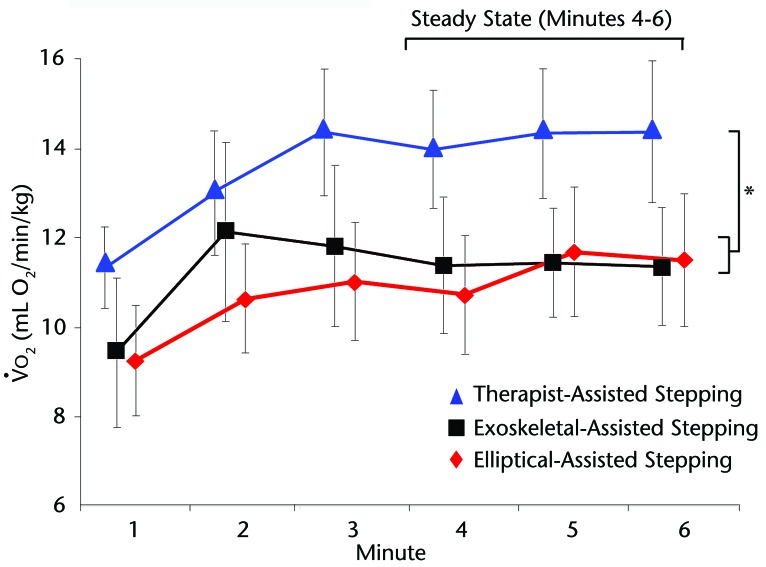
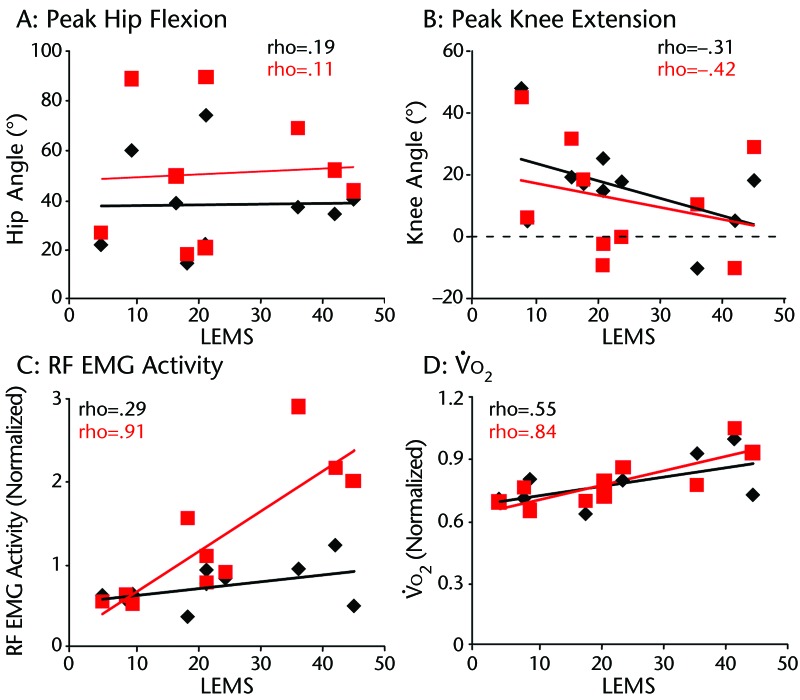
Results: Exoskeletal stepping kinematics closely approximated normal gait patterns, whereas significantly greater hip and knee flexion postures were observed during elliptical-assisted stepping. Measures of kinematic variability indicated consistent patterns in control participants and during exoskeletal-assisted stepping, whereas therapist- and elliptical-assisted stepping kinematics were more variable. Despite specific differences, EMG patterns generally were similar across stepping conditions in the participants with SCI. In contrast, oxygen consumption was consistently greater during therapist-assisted stepping. Limitations Limitations included a small sample size, lack of ability to evaluate kinetics during stepping, unilateral EMG recordings, and sagittal-plane kinematics.
Conclusions: Despite specific differences in kinematics and EMG activity, metabolic activity was similar during stepping in each robotic device. Understanding potential differences and similarities in stepping performance with robotic assistance may be important in delivery of repeated locomotor training using robotic or therapist assistance and for consumers of robotic devices.
Figures
References
-
- Behrman A, Harkema S. Locomotor training after human spinal cord injury: a series of case studies. Phys Ther. 2000;80:688–700 - PubMed
-
- Behrman A, Lawless-Dixon AR, Davis SB, et al. Locomotor training progression and outcomes after incomplete spinal cord injury. Phys Ther. 2005;85:1356–1371 - PubMed
-
- Hesse S, Bertelt C, Jahnke MT, et al. Treadmill training with partial body weight support compared with physiotherapy in nonambulatory hemiparetic patients. Stroke. 1995;26:976–981 - PubMed
-
- Macko RF, Ivey FM, Forrester LW, et al. Treadmill exercise rehabilitation improves ambulatory function and cardiovascular fitness in patients with chronic stroke: a randomized, controlled trial. Stroke. 2005;36:2206–2211 - PubMed
-
- Moore JL, Roth EJ, Killian C, Hornby TG. Locomotor training improves daily stepping activity and gait efficiency in individuals poststroke who have reached a “plateau” in recovery. Stroke. 2010;41:129–135 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
