

Does nonpayment for hospital-acquired catheter-associated urinary tract infections lead to overtesting and increased antimicrobial prescribing?
- PMID: 22700826
- PMCID: PMC3657518
- DOI: 10.1093/cid/cis556
Does nonpayment for hospital-acquired catheter-associated urinary tract infections lead to overtesting and increased antimicrobial prescribing?
Erratum in
- Clin Infect Dis. 2013 Mar;56(6):911-2
Abstract
Background: On 1 October 2008, in an effort to stimulate efforts to prevent catheter-associated urinary tract infection (CAUTI), the Centers for Medicare & Medicaid Services (CMS) implemented a policy of not reimbursing hospitals for hospital-acquired CAUTI. Since any urinary tract infection present on admission would not fall under this initiative, concerns have been raised that the policy may encourage more testing for and treatment of asymptomatic bacteriuria.
Methods: We conducted a retrospective multicenter cohort study with time series analysis of all adults admitted to the hospital 16 months before and 16 months after policy implementation among participating Society for Healthcare Epidemiology of America Research Network hospitals. Our outcomes were frequency of urine culture on admission and antimicrobial use.
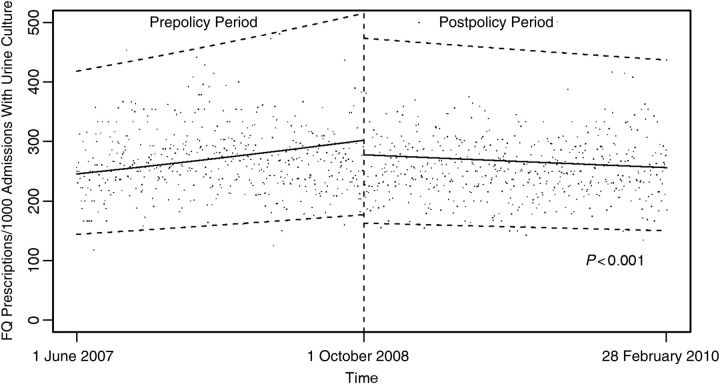
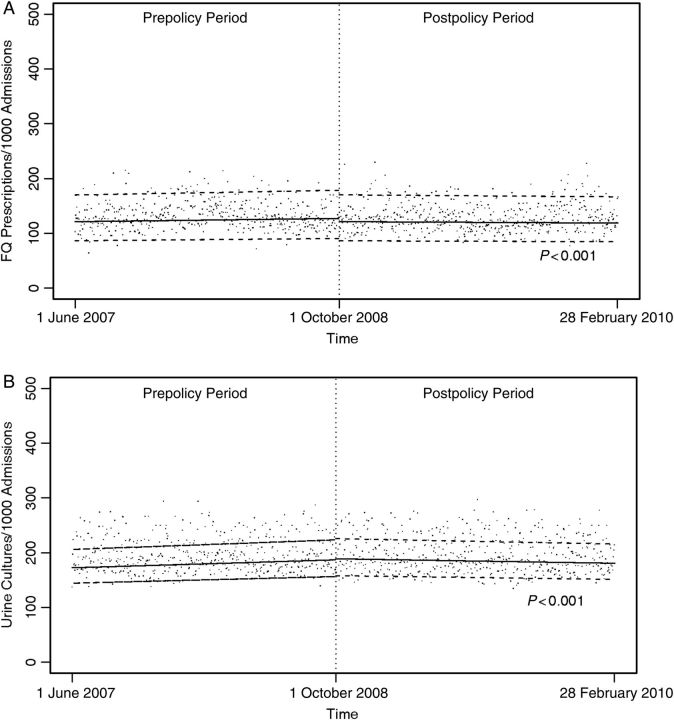
Results: A total of 39 hospitals from 22 states submitted data on 2 362 742 admissions. In 35 hospitals affected by the CMS policy, the median frequency of urine culture performance did not change after CMS policy implementation (19.2% during the prepolicy period vs 19.3% during the postpolicy period). The rate of change in urine culture performance increased minimally during the prepolicy period (0.5% per month) and decreased slightly during the postpolicy period (-0.25% per month; P < .001). In the subset of 10 hospitals providing antimicrobial use data, the median frequency of fluoroquinolone antimicrobial use did not change substantially (14.6% during the prepolicy period vs 14.0% during the postpolicy period). The rate of change in fluoroquinolone use increased during the prepolicy period (1.26% per month) and decreased during the postpolicy period (-0.60% per month; P < .001).
Conclusions: We found no evidence that CMS nonpayment policy resulted in overtesting to screen for and document a diagnosis of urinary tract infection as present on admission.
Figures
References
-
- Centers for Medicare and Medicaid Services (CMS), HHS. Medicare program; changes to the hospital inpatient prospective payment systems and fiscal year 2008 rates. Fed Regist. 2007;72:47129–8175. - PubMed
-
- Wald HL, Kramer AM. Nonpayment for harms resulting from medical care. JAMA. 2007;298:2782–4. - PubMed
-
- Wachter RM, Flanders SA, Fee C, Pronovost PJ. Public reporting of antibiotic timing in patients with pneumonia: lessons from a flawed performance measure. Ann Intern Med. 2008;149:29. - PubMed
-
- Nicolle LE, Bradley S, Colgan R, et al. Infectious Diseases Society of America guidelines for the diagnosis and treatment of asymptomatic bacteriuria in adults. Clin Infect Dis. 2005;40:643–54. doi:10.1086/427507. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
