

Relationships between levels of urinary podocalyxin, number of urinary podocytes, and histologic injury in adult patients with IgA nephropathy
- PMID: 22700887
- PMCID: PMC3430952
- DOI: 10.2215/CJN.08110811
Relationships between levels of urinary podocalyxin, number of urinary podocytes, and histologic injury in adult patients with IgA nephropathy
Abstract
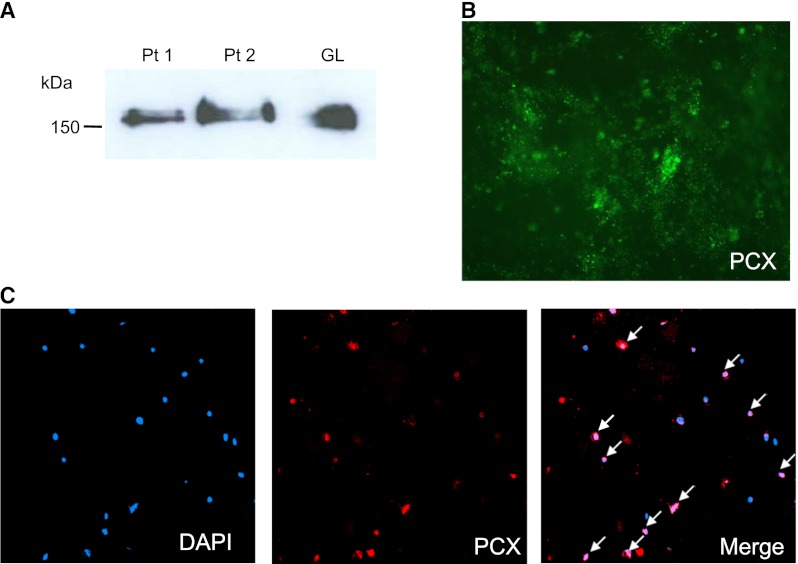
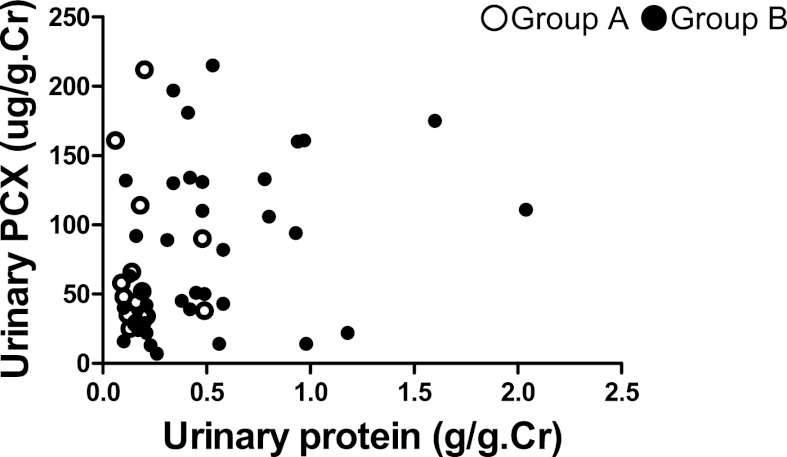
Background and objectives: Podocalyxin (PCX) is present on the apical cell membrane of podocytes and is shed in urine from injured podocytes. Urinary podocalyxin (u-PCX) is associated with severity of active glomerular injury in patients with glomerular diseases. This study examined the relationship between number of urinary podocytes, levels of u-PCX, and glomerular injury in adults with IgA nephropathy (IgAN).
Design, setting, participants, & measurements: Urine samples voided in the morning on the day of biopsy were obtained from 51 patients with IgAN (18 men and 33 women; mean age, 31 years). All renal biopsy specimens were analyzed histologically. Pathologic variables of IgAN were analyzed per Shigematsu classification, the Oxford classification of IgAN, and the Clinical Guidelines of IgAN in Japan. Levels of u-PCX were measured by sandwich ELISA.
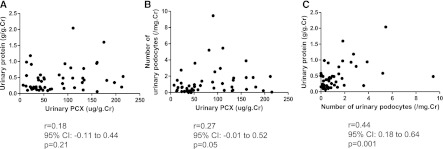
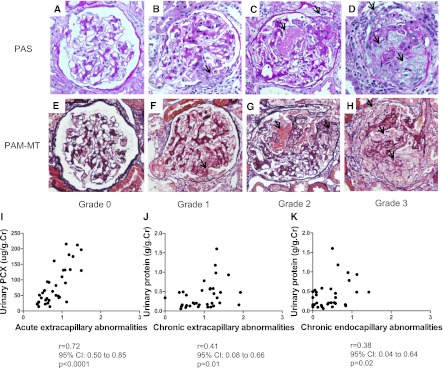
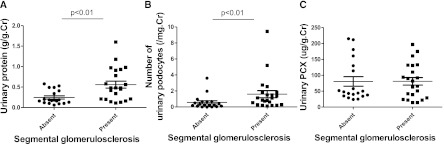
Results: Histologic analysis based on Shigematsu classification revealed a significant correlation between levels of u-PCX and severity of acute extracapillary abnormalities (r=0.72; P<0.001), but levels of urinary protein excretion did not correlate with acute glomerular abnormalities. Levels of urinary protein excretion in patients with segmental sclerosis (n=19) were higher than in patients without (n=22) (0.49 [interquartile range (IQR), 0.20-0.88] g/g creatinine versus 0.20 [IQR, 0.10-0.33] g/g creatinine; P<0.01). The number of urinary podocytes in patients with segmental sclerosis was higher than in patients without (1.05 [IQR, 0.41-1.67] per mg creatinine versus 0.28 [IQR, 0.10-0.66] per mg creatinine; P<0.01).
Conclusions: Levels of u-PCX and the number of urinary podocytes are associated with histologic abnormalities in adults with IgAN.
Figures
Similar articles
-
Evaluation of renal clinicopathological changes in IgA nephropathy by urinary podocytes excretion and podocalyxin expression.Ren Fail. 2012;34(7):821-6. doi: 10.3109/0886022X.2011.643352. Epub 2012 Jun 8. Ren Fail. 2012. PMID: 22679920
-
Urinary podocyte can be an indicator for the pathogenetic condition of patients with IgA nephropathy.Clin Lab. 2014;60(10):1709-15. doi: 10.7754/clin.lab.2014.131225. Clin Lab. 2014. PMID: 25651718
-
Urinary podocalyxin, the novel biomarker for detecting early renal change in obesity.J Nephrol. 2016 Feb;29(1):37-44. doi: 10.1007/s40620-015-0199-8. Epub 2015 Apr 24. J Nephrol. 2016. PMID: 25905599
-
The implications of focal segmental glomerulosclerosis in children with IgA nephropathy.Pediatr Nephrol. 2020 Nov;35(11):2043-2047. doi: 10.1007/s00467-019-04414-4. Epub 2019 Nov 26. Pediatr Nephrol. 2020. PMID: 31773265 Review.
-
Urine markers of podocyte dysfunction: a review of podocalyxin and nephrin in selected glomerular diseases.Biomark Med. 2018 Aug;12(8):927-935. doi: 10.2217/bmm-2018-0152. Epub 2018 Jul 6. Biomark Med. 2018. PMID: 29976076 Review.
Cited by
-
Exfoliated Kidney Cells from Urine for Early Diagnosis and Prognostication of CKD: The Way of the Future?Int J Mol Sci. 2022 Jul 9;23(14):7610. doi: 10.3390/ijms23147610. Int J Mol Sci. 2022. PMID: 35886957 Free PMC article. Review.
-
Biomarkers in IgA nephropathy: relationship to pathogenetic hits.Expert Opin Med Diagn. 2013 Nov;7(6):615-27. doi: 10.1517/17530059.2013.856878. Expert Opin Med Diagn. 2013. PMID: 24175678 Free PMC article. Review.
-
Kidney transplant monitoring by urinary flow cytometry: Biomarker combination of T cells, renal tubular epithelial cells, and podocalyxin-positive cells detects rejection.Sci Rep. 2020 Jan 21;10(1):796. doi: 10.1038/s41598-020-57524-7. Sci Rep. 2020. PMID: 31964937 Free PMC article.
-
Identification of novel molecular signatures of IgA nephropathy through an integrative -omics analysis.Sci Rep. 2017 Aug 22;7(1):9091. doi: 10.1038/s41598-017-09393-w. Sci Rep. 2017. PMID: 28831120 Free PMC article.
-
TWEAK/Fn14 system and crescent formation in IgA nephropathy.BMC Nephrol. 2015 Mar 14;16:27. doi: 10.1186/s12882-015-0022-8. BMC Nephrol. 2015. PMID: 25885587 Free PMC article.
References
-
- Kriz W, Gretz N, Lemley KV: Progression of glomerular diseases: Is the podocyte the culprit? Kidney Int 54: 687–697, 1998 - PubMed
-
- Mundel P, Shankland SJ: Podocyte biology and response to injury. J Am Soc Nephrol 13: 3005–3015, 2002 - PubMed
-
- Asanuma K, Yanagida-Asanuma E, Takagi M, Kodama F, Tomino Y: The role of podocytes in proteinuria. Nephrology (Carlton) 12[Suppl 3]: S15–S20, 2007 - PubMed
-
- Hara M, Yanagihara T, Kihara I: Cumulative excretion of urinary podocytes reflects disease progression in IgA nephropathy and Schönlein-Henoch purpura nephritis. Clin J Am Soc Nephrol 2: 231–238, 2007 - PubMed
-
- Hara M, Yanagihara T, Takada T, Itoh M, Matsuno M, Yamamoto T, Kihara I: Urinary excretion of podocytes reflects disease activity in children with glomerulonephritis. Am J Nephrol 18: 35–41, 1998 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
