

Cell carriage, delivery, and selective replication of an oncolytic virus in tumor in patients
- PMID: 22700953
- PMCID: PMC3893925
- DOI: 10.1126/scitranslmed.3003578
Cell carriage, delivery, and selective replication of an oncolytic virus in tumor in patients
Abstract
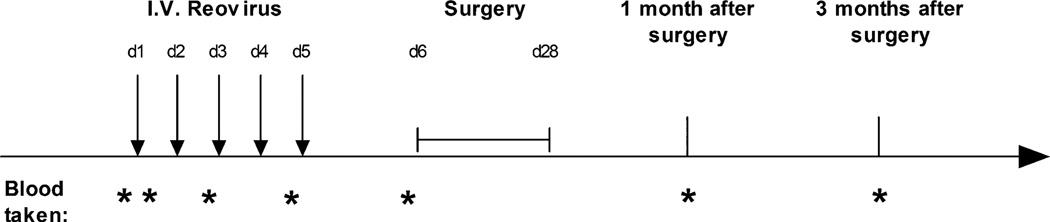
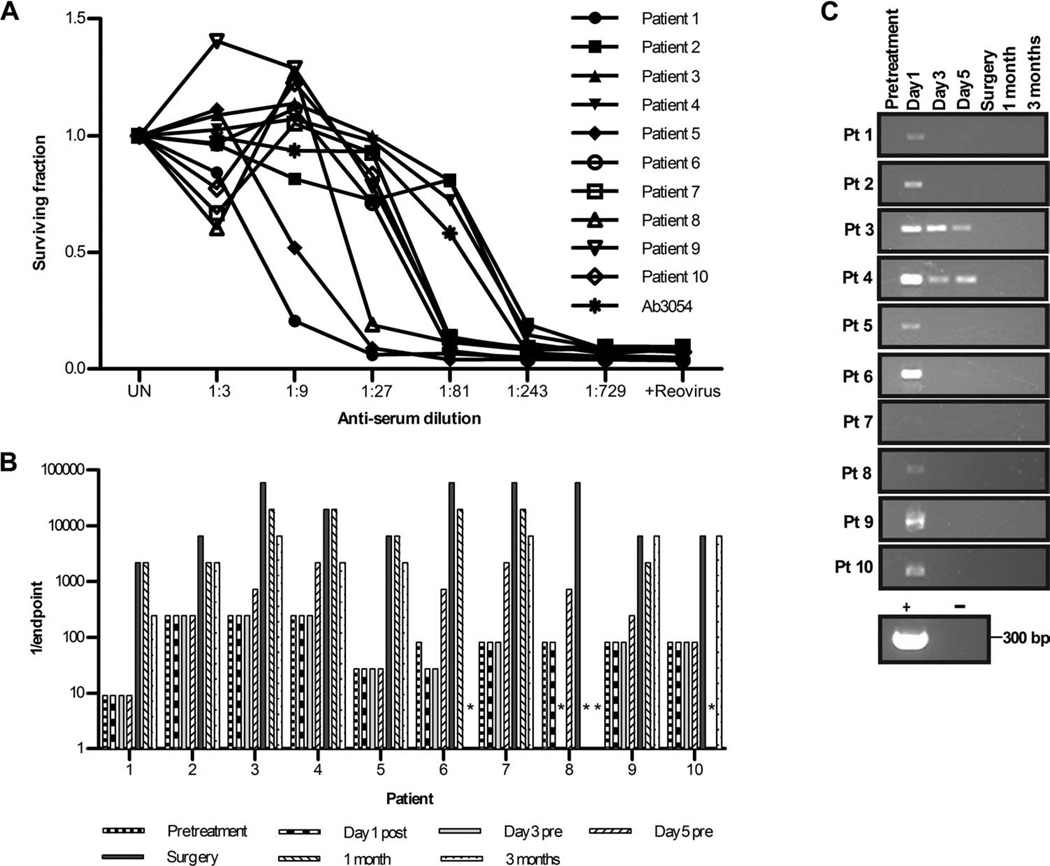
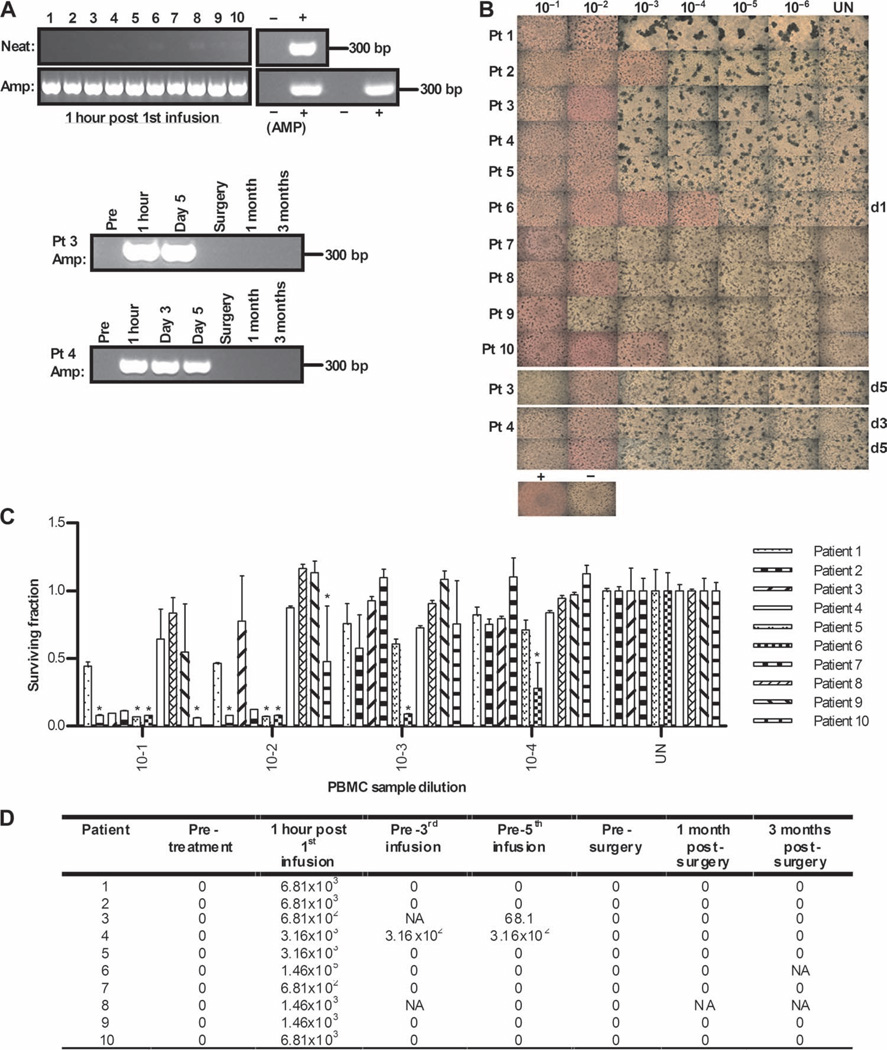
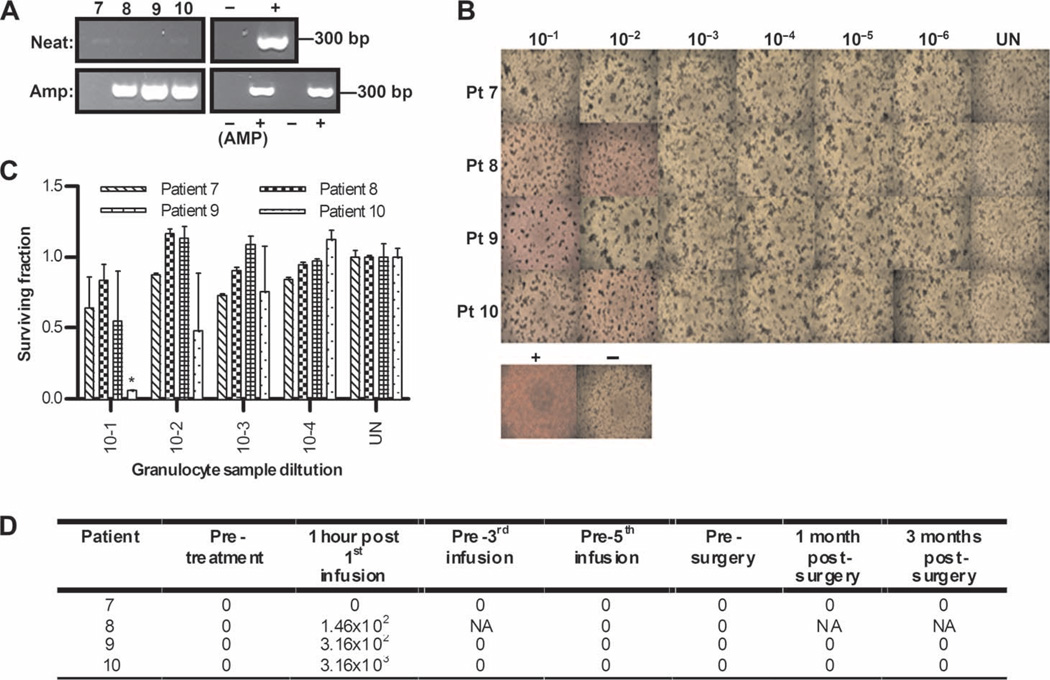
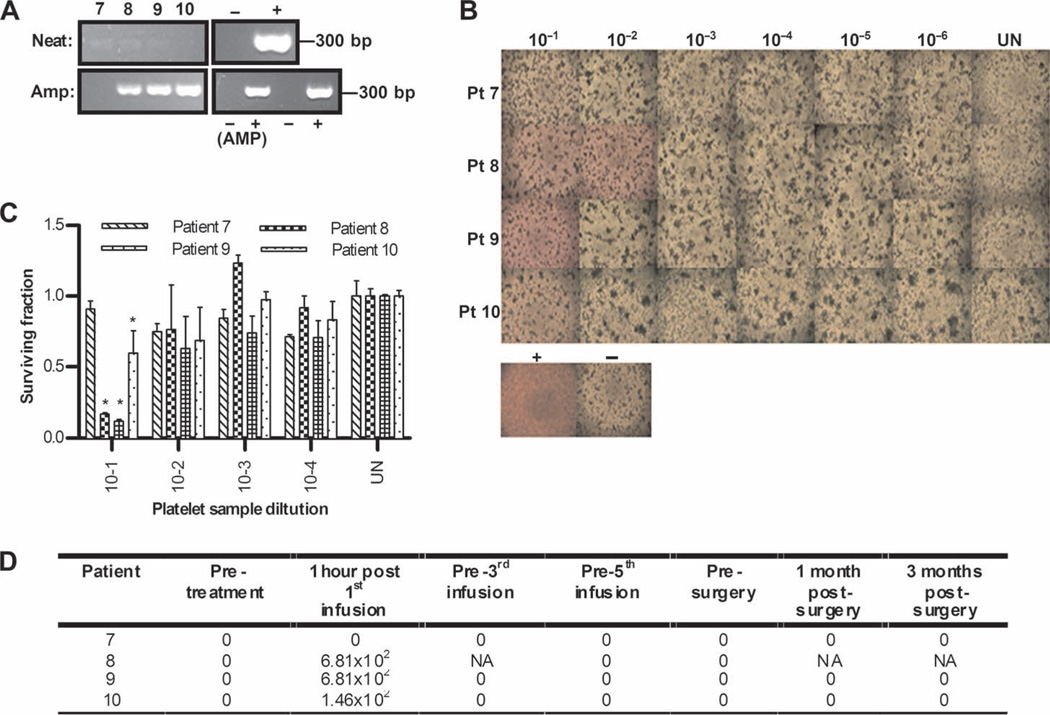
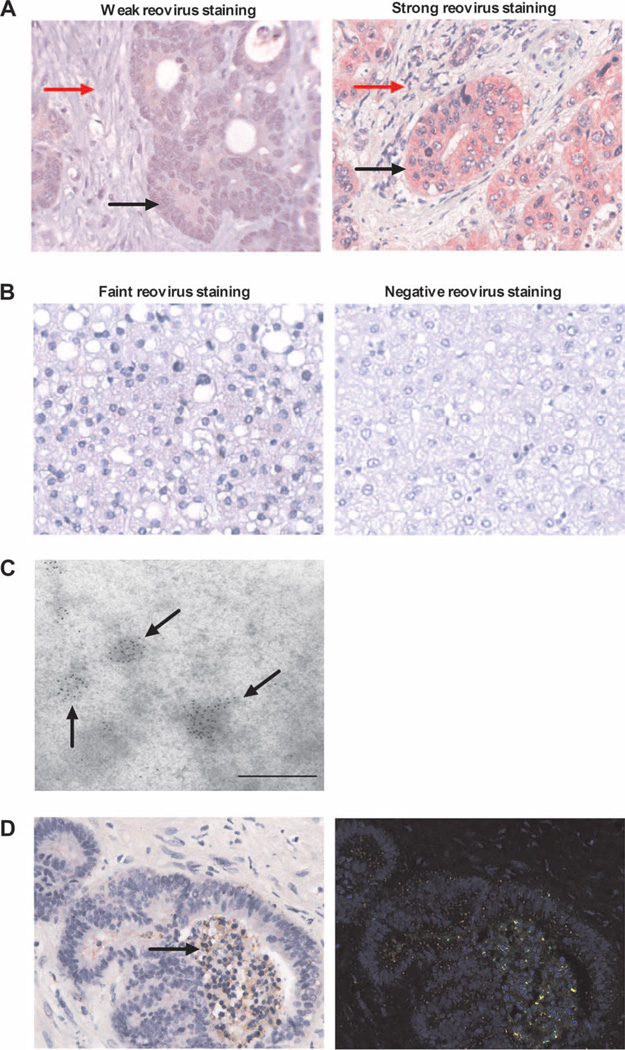
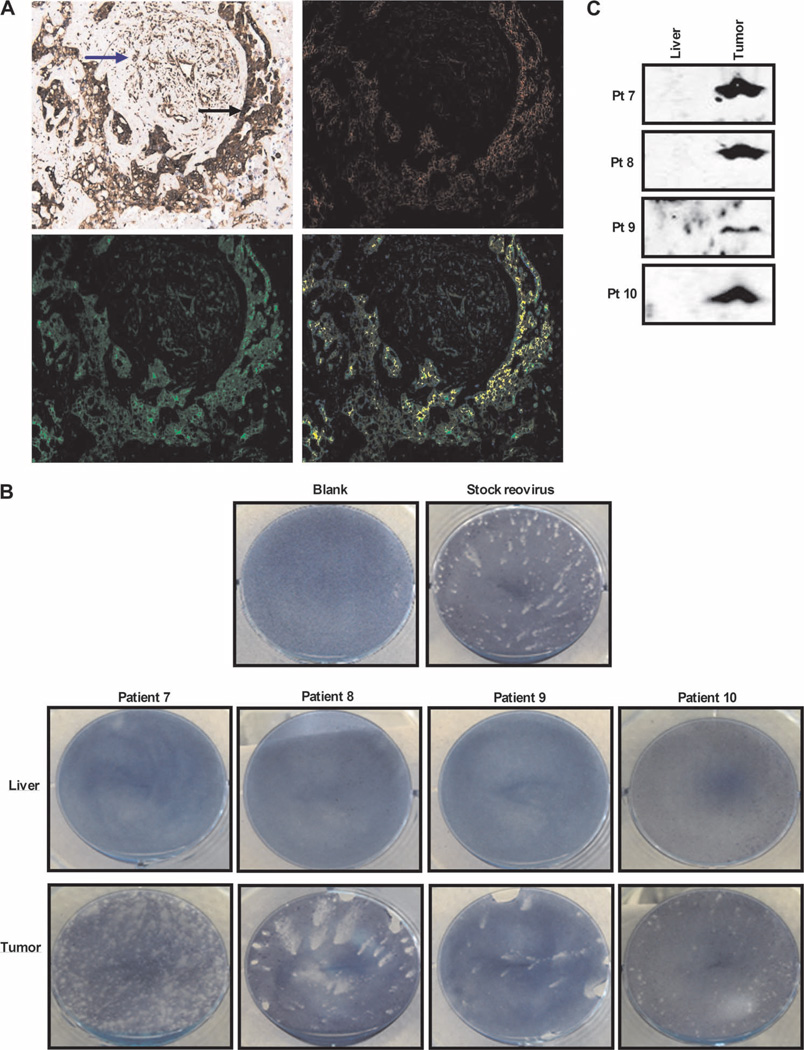
Oncolytic viruses, which preferentially lyse cancer cells and stimulate an antitumor immune response, represent a promising approach to the treatment of cancer. However, how they evade the antiviral immune response and their selective delivery to, and replication in, tumor over normal tissue has not been investigated in humans. Here, we treated patients with a single cycle of intravenous reovirus before planned surgery to resect colorectal cancer metastases in the liver. Tracking the viral genome in the circulation showed that reovirus could be detected in plasma and blood mononuclear, granulocyte, and platelet cell compartments after infusion. Despite the presence of neutralizing antibodies before viral infusion in all patients, replication-competent reovirus that retained cytotoxicity was recovered from blood cells but not plasma, suggesting that transport by cells could protect virus for potential delivery to tumors. Analysis of surgical specimens demonstrated greater, preferential expression of reovirus protein in malignant cells compared to either tumor stroma or surrounding normal liver tissue. There was evidence of viral factories within tumor, and recovery of replicating virus from tumor (but not normal liver) was achieved in all four patients from whom fresh tissue was available. Hence, reovirus could be protected from neutralizing antibodies after systemic administration by immune cell carriage, which delivered reovirus to tumor. These findings suggest new preclinical and clinical scheduling and treatment combination strategies to enhance in vivo immune evasion and effective intravenous delivery of oncolytic viruses to patients in vivo.
Figures
References
-
- Garcia-Aragoncillo E, Hernandez-Alcoceba R. Design of virotherapy for effective tumor treatment. Curr. Opin. Mol. Ther. 2010;12:403–411. - PubMed
-
- Eager RM, Nemunaitis J. Clinical development directions in oncolytic viral therapy. Cancer Gene Ther. 2011;18:305–317. - PubMed
-
- Kaufman HL, Bines SD. OPTIM trial: A phase III trial of an oncolytic herpes virus encoding GM-CSF for unresectable stage III or IV melanoma. Future Oncol. 2010;6:941–949. - PubMed
-
- Breitbach CJ, Thorne SH, Bell JC, Kirn DH. Targeted and armed oncolytic poxviruses for cancer: The lead example of JX-594. Curr. Pharm. Biotechnol. 2011 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
