

Hyperglycemia increases muscle blood flow and alters endothelial function in adolescents with type 1 diabetes
- PMID: 22701470
- PMCID: PMC3371684
- DOI: 10.1155/2012/170380
Hyperglycemia increases muscle blood flow and alters endothelial function in adolescents with type 1 diabetes
Abstract
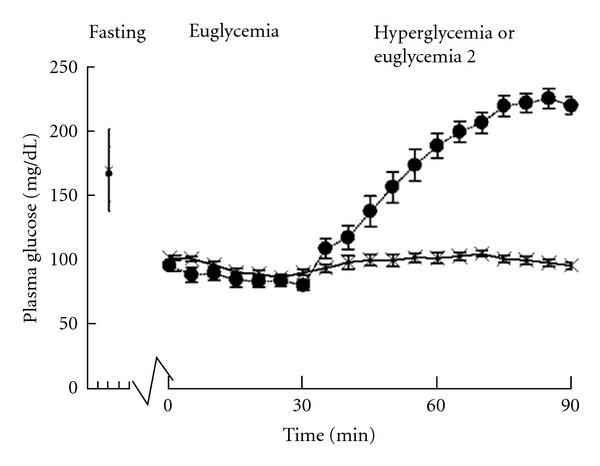
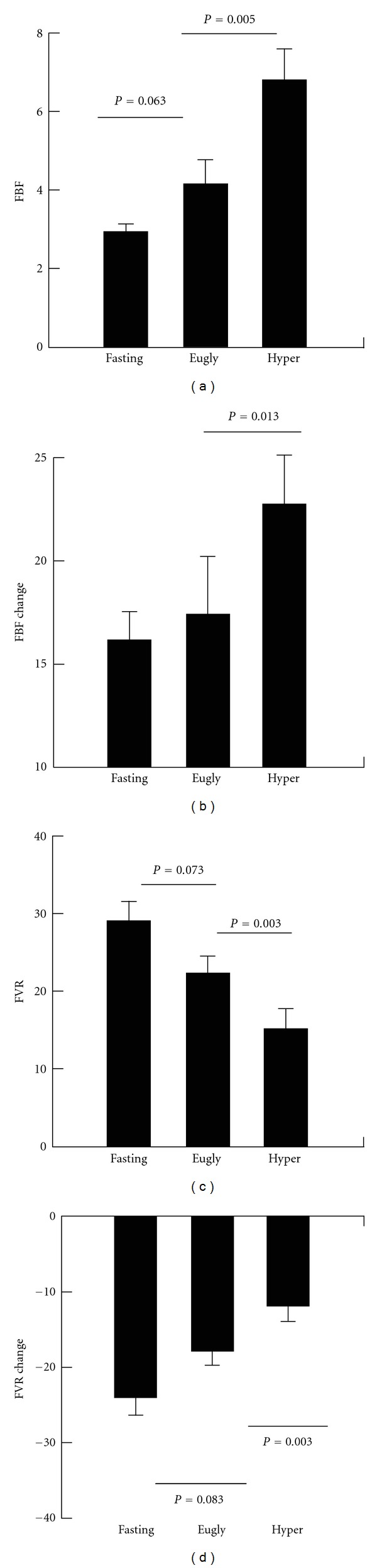
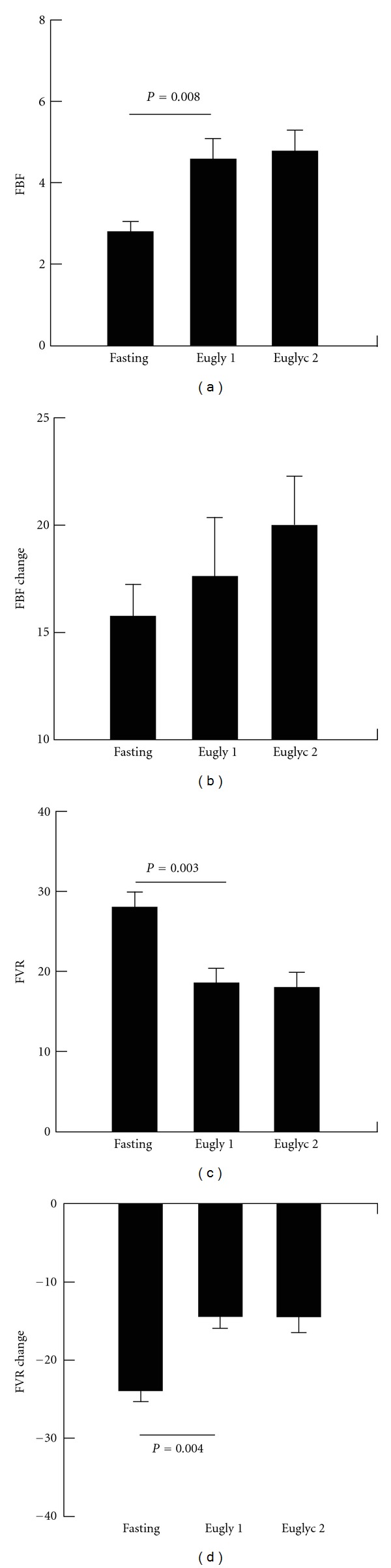
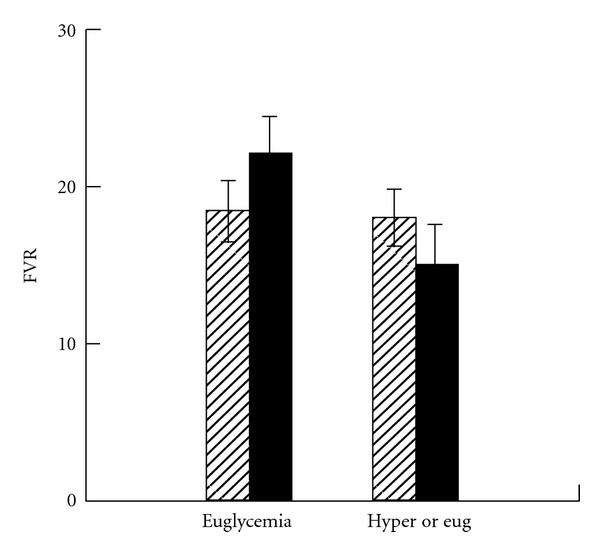
Alterations of blood flow and endothelial function precede development of complications in type 1 diabetes. The effects of hyperglycemia on vascular function in early type 1 diabetes are poorly understood. To investigate the effect of hyperglycemia on forearm vascular resistance (FVR) and endothelial function in adolescents with type 1 diabetes, FVR was measured before and after 5 minutes of upper arm arterial occlusion using venous occlusion plethysmography in (1) fasted state, (2) euglycemic state (~90 mg/dL; using 40 mU/m(2)/min insulin infusion), and (3) hyperglycemic state (~200 mg/dL) in 11 adolescents with type 1 diabetes. Endothelial function was assessed by the change in FVR following occlusion. Seven subjects returned for a repeat study with hyperglycemia replaced by euglycemia. Preocclusion FVR decreased from euglycemia to hyperglycemia (P = 0.003). Postocclusion fall in FVR during hyperglycemia was less than during euglycemia (P = 0.002). These findings were not reproduced when hyperglycemia was replaced with a second euglycemia. These results demonstrate that acute hyperglycemia causes vasodilation and alters endothelial function in adolescents with type 1 diabetes. In addition they have implications for future studies of endothelial function in type 1 diabetes and provide insight into the etiology of macrovascular and microvascular complications of type 1 diabetes.
Figures
Similar articles
-
Ascorbic acid blocks hyperglycemic impairment of endothelial function in adolescents with type 1 diabetes.Pediatr Diabetes. 2012 Dec;13(8):607-10. doi: 10.1111/j.1399-5448.2012.00882.x. Epub 2012 Aug 28. Pediatr Diabetes. 2012. PMID: 22925199 Free PMC article.
-
Effects of acute hyperglycemia on endothelium-dependent vasodilation in patients with diabetes mellitus or impaired glucose metabolism.Endothelium. 2003;10(2):65-70. doi: 10.1080/10623320303362. Endothelium. 2003. PMID: 12791513
-
Forearm vascular control during acute hyperglycemia in healthy humans.Am J Physiol Endocrinol Metab. 2004 Mar;286(3):E472-80. doi: 10.1152/ajpendo.00348.2003. Epub 2003 Oct 28. Am J Physiol Endocrinol Metab. 2004. PMID: 14583439 Clinical Trial.
-
Vascular endothelial dysfunction and nutritional compounds in early type 1 diabetes.Curr Diabetes Rev. 2014 May;10(3):201-7. doi: 10.2174/1573399810666140613124326. Curr Diabetes Rev. 2014. PMID: 24925525 Review.
-
Endothelial dysfunction in diabetes mellitus.Vasc Health Risk Manag. 2007;3(6):853-76. Vasc Health Risk Manag. 2007. PMID: 18200806 Free PMC article. Review.
Cited by
-
Hyperglycemic endothelial dysfunction: does it happen and does it matter?J Thorac Dis. 2015 Oct;7(10):1693-5. doi: 10.3978/j.issn.2072-1439.2015.10.24. J Thorac Dis. 2015. PMID: 26623085 Free PMC article. No abstract available.
-
ISPAD Clinical Practice Consensus Guidelines 2018: Microvascular and macrovascular complications in children and adolescents.Pediatr Diabetes. 2018 Oct;19 Suppl 27(Suppl 27):262-274. doi: 10.1111/pedi.12742. Pediatr Diabetes. 2018. PMID: 30079595 Free PMC article. No abstract available.
-
Increased Pre- and Post-Meal Free Fatty Acid Levels in Black, Obese Adolescents.Metab Syndr Relat Disord. 2016 Sep;14(7):340-6. doi: 10.1089/met.2015.0122. Epub 2016 Jul 15. Metab Syndr Relat Disord. 2016. PMID: 27419255 Free PMC article.
-
The role of blood pressure in risk of ischemic and hemorrhagic stroke in type 1 diabetes.Cardiovasc Diabetol. 2019 Jul 9;18(1):88. doi: 10.1186/s12933-019-0891-4. Cardiovasc Diabetol. 2019. PMID: 31288813 Free PMC article.
-
Effects of glucose control and variability on endothelial function and repair in adolescents with type 1 diabetes.ISRN Endocrinol. 2013 Dec 29;2013:876547. doi: 10.1155/2013/876547. eCollection 2013. ISRN Endocrinol. 2013. PMID: 24490081 Free PMC article.
References
-
- McGill HC, Jr., McMahan CA, Herderick EE, Malcom GT, Tracy RE, Jack P. Origin of atherosclerosis in childhood and adolescence. American Journal of Clinical Nutrition. 2000;72(5):1307S–1315S. - PubMed
-
- Stehouwer CDA, Lambert J, Donker AJM, van Hinsbergh VWM. Endothelial dysfunction and pathogenesis of diabetic angiopathy. Cardiovascular Research. 1997;34(1):55–68. - PubMed
-
- Berenson GS. Childhood risk factors predict adult risk associated with subclinical cardiovascular disease: the Bogalusa Heart study. American Journal of Cardiology. 2002;90(10):3L–7L. - PubMed
-
- Donaghue KC, Robinson J, McCredie R, Fung A, Silink M, Celermajer DS. Large vessel dysfunction in diabetic adolescents and its relationship to small vessel complications. Journal of Pediatric Endocrinology and Metabolism. 1997;10(6):593–598. - PubMed
-
- Wiltshire EJ, Gent R, Hirte C, Pena A, Thomas DW, Couper JJ. Endothelial dysfunction relates to folate status in children and adolescents with type 1 diabetes. Diabetes. 2002;51(7):2282–2286. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials