

Ultrahigh-field MRI in human ischemic stroke--a 7 tesla study
- PMID: 22701525
- PMCID: PMC3365122
- DOI: 10.1371/journal.pone.0037631
Ultrahigh-field MRI in human ischemic stroke--a 7 tesla study
Abstract
Introduction: Magnetic resonance imaging (MRI) using field strengths up to 3 Tesla (T) has proven to be a powerful tool for stroke diagnosis. Recently, ultrahigh-field (UHF) MRI at 7 T has shown relevant diagnostic benefits in imaging of neurological diseases, but its value for stroke imaging has not been investigated yet. We present the first evaluation of a clinically feasible stroke imaging protocol at 7 T. For comparison an established stroke imaging protocol was applied at 3 T.
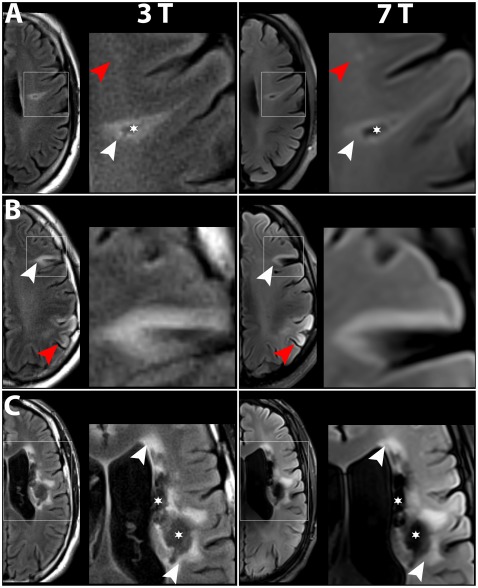
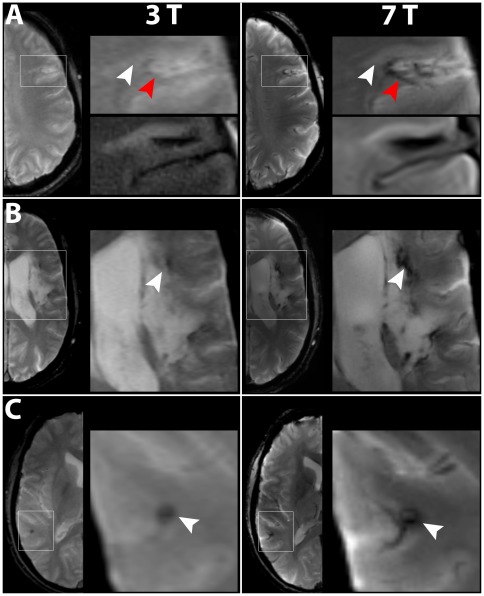
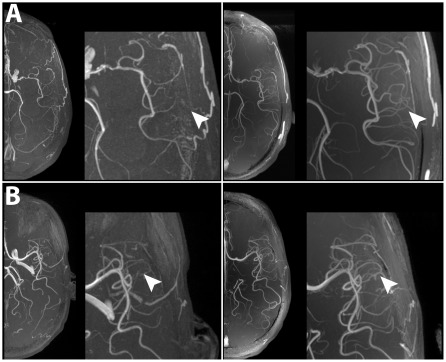
Methods: In a prospective imaging study seven patients with subacute and chronic stroke were included. Imaging at 3 T was immediately followed by 7 T imaging. Both protocols included T1-weighted 3D Magnetization-Prepared Rapid-Acquired Gradient-Echo (3D-MPRAGE), T2-weighted 2D Fluid Attenuated Inversion Recovery (2D-FLAIR), T2-weighted 2D Fluid Attenuated Inversion Recovery (2D-T2-TSE), T2* weighted 2D Fast Low Angle Shot Gradient Echo (2D-HemoFLASH) and 3D Time-of-Flight angiography (3D-TOF).
Results: The diagnostic information relevant for clinical stroke imaging obtained at 3 T was equally available at 7 T. Higher spatial resolution at 7 T revealed more anatomical details precisely depicting ischemic lesions and periinfarct alterations. A clear benefit in anatomical resolution was also demonstrated for vessel imaging at 7 T. RF power deposition constraints induced scan time prolongation and reduced brain coverage for 2D-FLAIR, 2D-T2-TSE and 3D-TOF at 7 T versus 3 T.
Conclusions: The potential of 7 T MRI for human stroke imaging is shown. Our pilot study encourages a further evaluation of the diagnostic benefit of stroke imaging at 7 T in a larger study.
Conflict of interest statement
Figures


References
-
- Merino JG, Warach S. Imaging of acute stroke. Nat Rev Neurol. 2010;6:560–571. doi: 10.1038/nrneurol.2010.129. - DOI - PubMed
-
- Lupo JM, Li Y, Hess CP, Nelson SJ. Advances in ultra-high field MRI for the clinical management of patients with brain tumors. Current Opinion in Neurology. 2011;24:605–615. doi: 10.1097/WCO.0b013e32834cd495. - DOI - PubMed
-
- Dammann P, Barth M, Zhu Y, Maderwald S, Schlamann M, et al. Susceptibility weighted magnetic resonance imaging of cerebral cavernous malformations: prospects, drawbacks, and first experience at ultra–high field strength (7-Tesla) magnetic resonance imaging. Neurosurgical FOCUS. 2010;29:E5. doi: 10.3171/2010.6.FOCUS10130. - DOI - PubMed
-
- Kwon D, Kim J, Oh S, Jeong H, Park S, et al. Seven-tesla magnetic resonance images of the substantia nigra in Parkinson disease. Annals of Neurology, Annals of Neurology 71, 71: 267, 267–277, 277. doi:10.1002/ 2012;ana.22592 10.1002/ana.22592. - PubMed
-
- Tallantyre EC, Dixon JE, Donaldson I, Owens T, Morgan PS, et al. Ultra-high-field imaging distinguishes MS lesions from asymptomatic white matter lesions. Neurology. 2011;76:534–539. doi: 10.1212/WNL.0b013e31820b7630. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
