

Preoperative multimodal motor mapping: a comparison of magnetoencephalography imaging, navigated transcranial magnetic stimulation, and direct cortical stimulation
- PMID: 22702484
- PMCID: PMC4060619
- DOI: 10.3171/2012.5.JNS112124
Preoperative multimodal motor mapping: a comparison of magnetoencephalography imaging, navigated transcranial magnetic stimulation, and direct cortical stimulation
Abstract
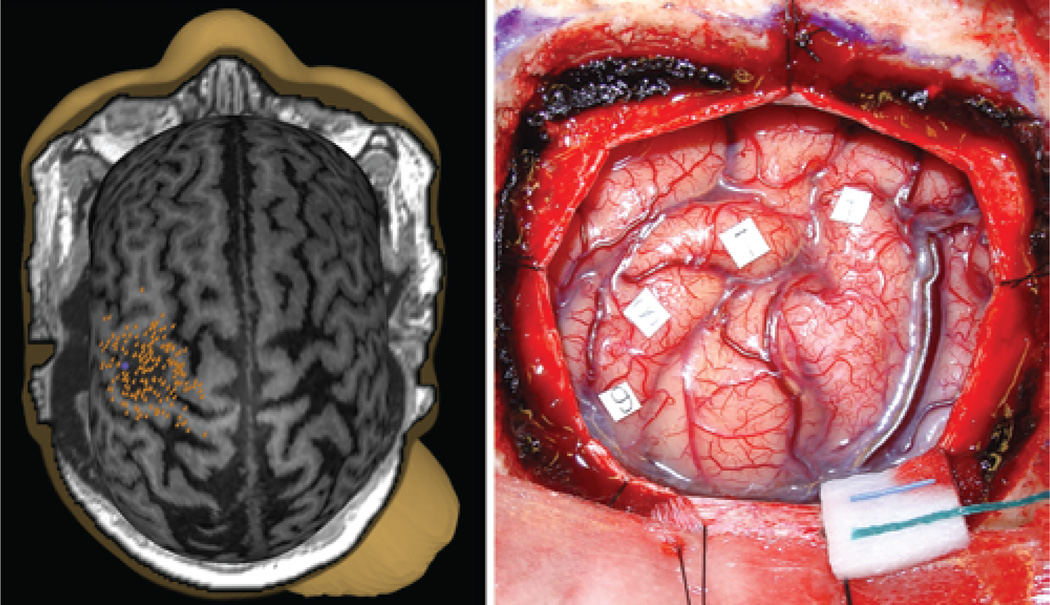
Object: Direct cortical stimulation (DCS) is the gold-standard technique for motor mapping during craniotomy. However, preoperative noninvasive motor mapping is becoming increasingly accurate. Two such noninvasive modalities are navigated transcranial magnetic stimulation (TMS) and magnetoencephalography (MEG) imaging. While MEG imaging has already been extensively validated as an accurate modality of noninvasive motor mapping, TMS is less well studied. In this study, the authors compared the accuracy of TMS to both DCS and MEG imaging.
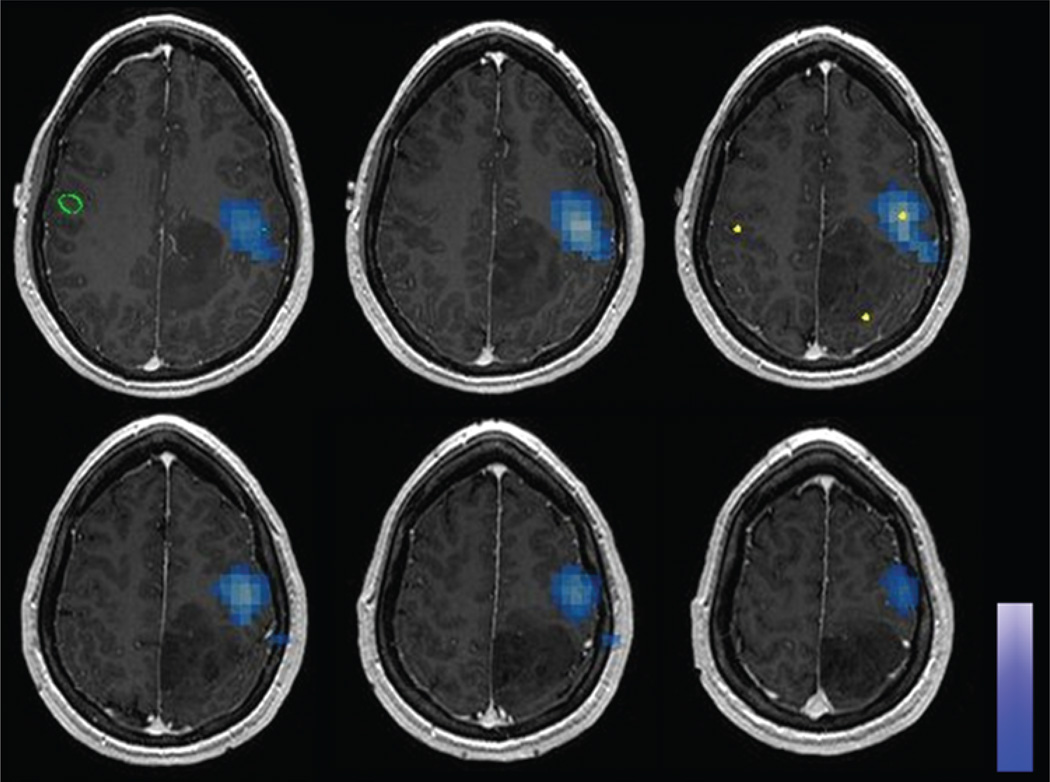
Methods: Patients with tumors in proximity to primary motor cortex underwent preoperative TMS and MEG imaging for motor mapping. The patients subsequently underwent motor mapping via intraoperative DCS. The loci of maximal response were recorded from each modality and compared. Motor strength was assessed at 3 months postoperatively.
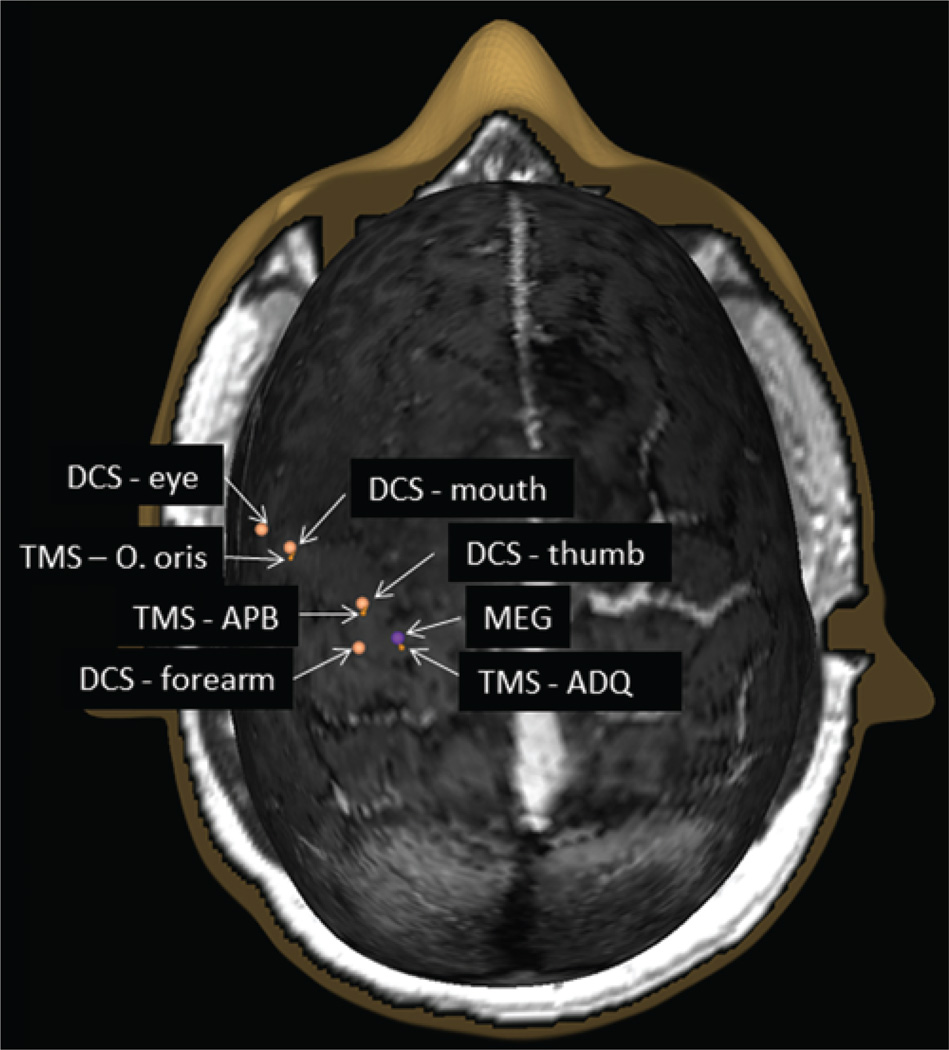
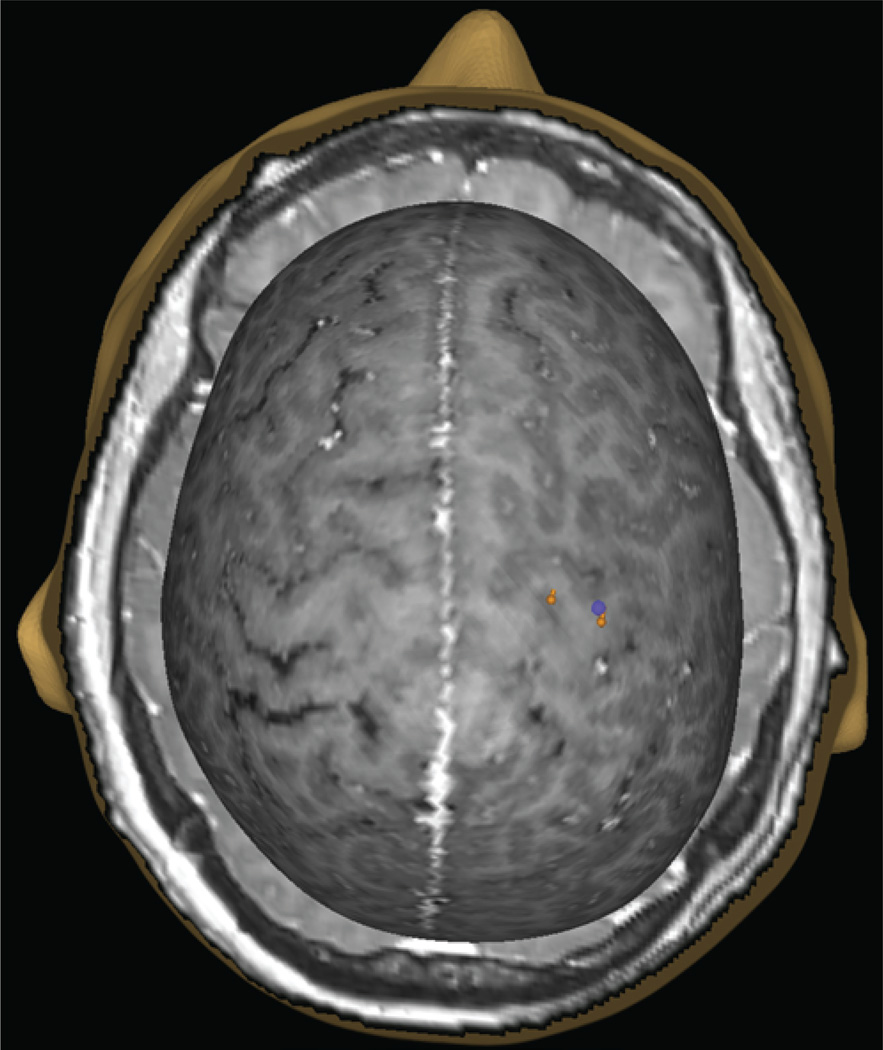
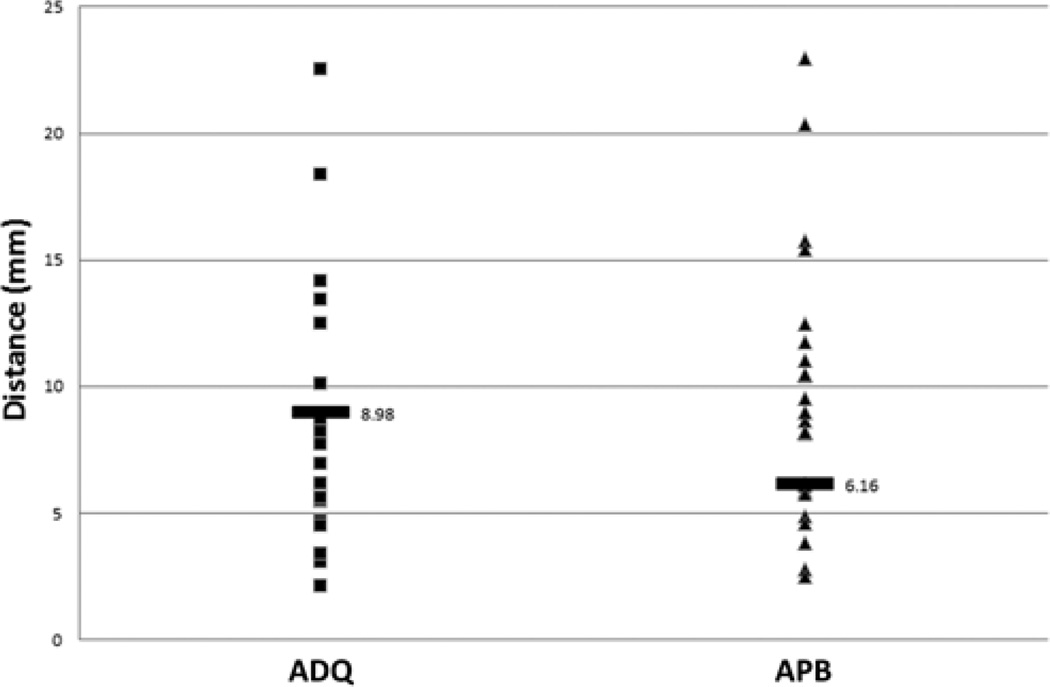
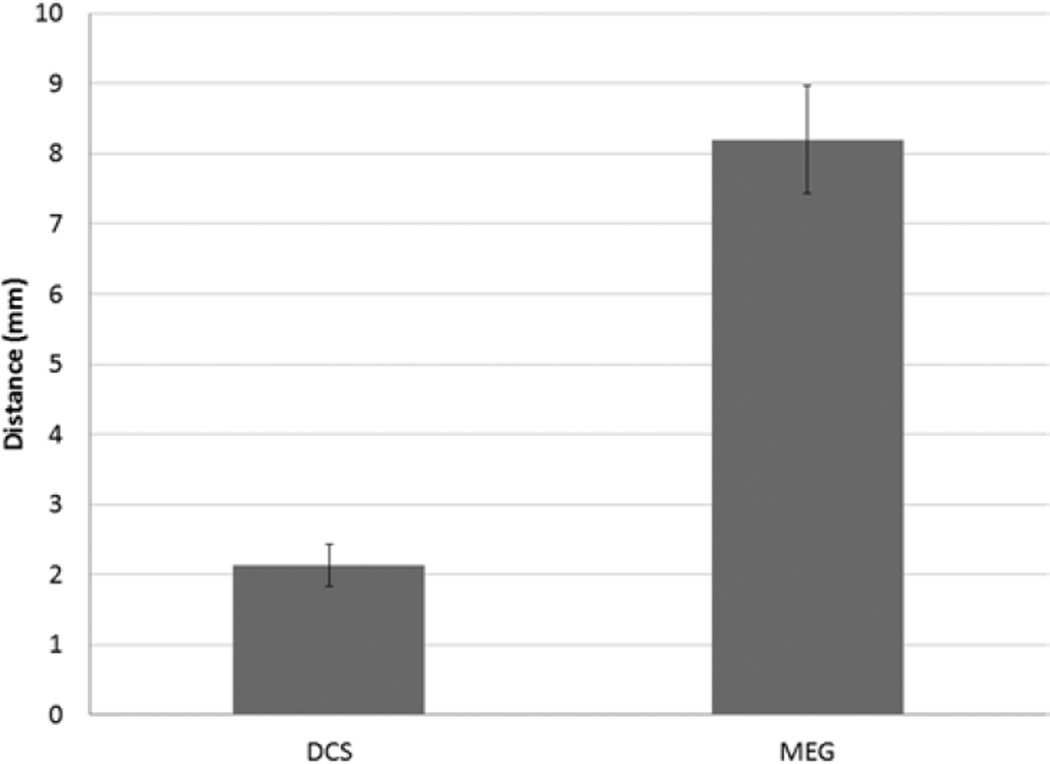
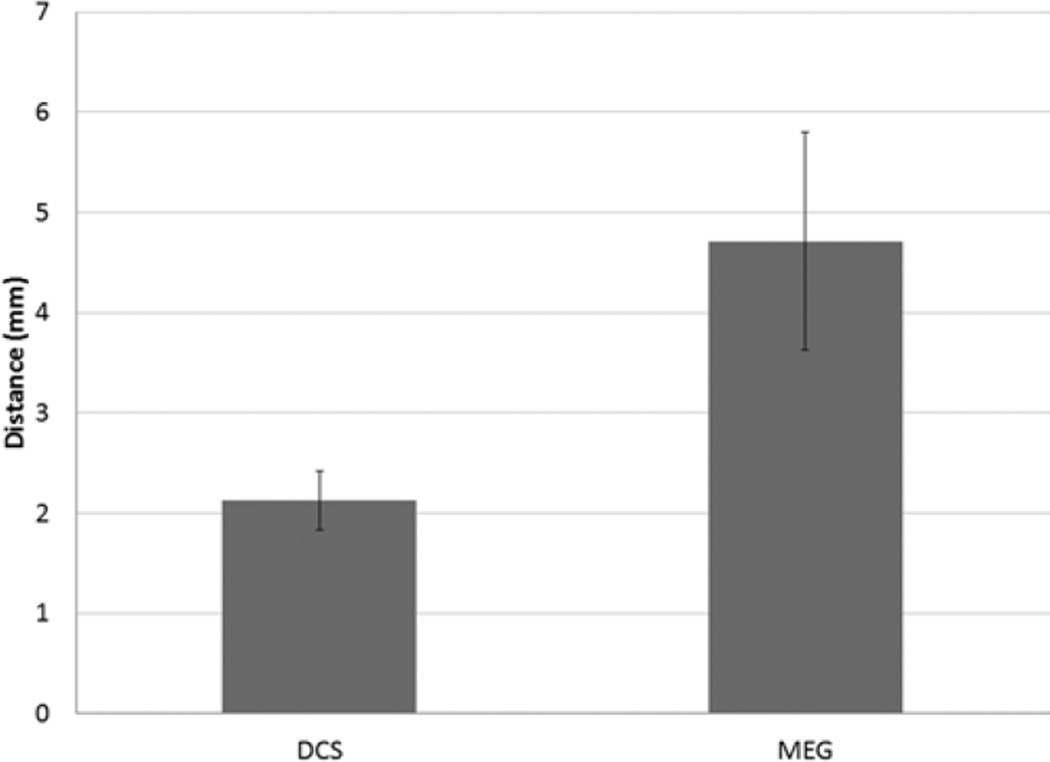
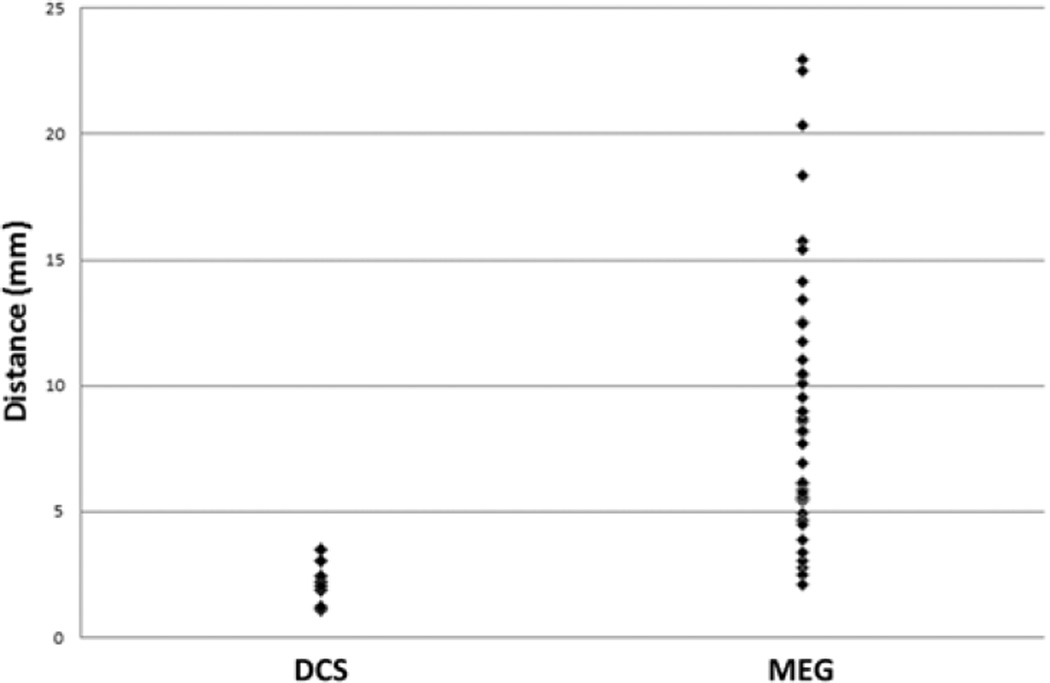
Results: Transcranial magnetic stimulation and MEG imaging were performed on 24 patients. Intraoperative DCS yielded 8 positive motor sites in 5 patients. The median distance ± SEM between TMS and DCS motor sites was 2.13 ± 0.29 mm, and between TMS and MEG imaging motor sites was 4.71 ± 1.08 mm. In no patients did DCS motor mapping reveal a motor site that was unrecognized by TMS. Three of 24 patients developed new, early neurological deficit in the form of upper-extremity paresis. At the 3-month follow-up evaluation, 2 of these patients were significantly improved, experiencing difficulty only with fine motor tasks; the remaining patient had improvement to 4/5 strength. There were no deaths over the course of the study.
Conclusions: Maps of the motor system generated with TMS correlate well with those generated by both MEG imaging and DCS. Negative TMS mapping also correlates with negative DCS mapping. Navigated TMS is an accurate modality for noninvasively generating preoperative motor maps.
Figures
Similar articles
-
Language mapping with navigated repetitive TMS: proof of technique and validation.Neuroimage. 2013 Nov 15;82:260-72. doi: 10.1016/j.neuroimage.2013.05.018. Epub 2013 May 20. Neuroimage. 2013. PMID: 23702420 Free PMC article.
-
Impairment of preoperative language mapping by lesion location: a functional magnetic resonance imaging, navigated transcranial magnetic stimulation, and direct cortical stimulation study.J Neurosurg. 2015 Aug;123(2):314-24. doi: 10.3171/2014.10.JNS141582. Epub 2015 Apr 17. J Neurosurg. 2015. PMID: 25884257
-
Combined noninvasive language mapping by navigated transcranial magnetic stimulation and functional MRI and its comparison with direct cortical stimulation.J Neurosurg. 2015 Jul;123(1):212-25. doi: 10.3171/2014.9.JNS14929. Epub 2015 Mar 6. J Neurosurg. 2015. PMID: 25748306
-
[Navigated transcranial magnetic stimulation for preoperative mapping of the eloquent cortex].Nervenarzt. 2015 Dec;86(12):1508-15. doi: 10.1007/s00115-015-4316-7. Nervenarzt. 2015. PMID: 26452779 Review. German.
-
[Presurgical functional magnetic resonance imaging].Radiologe. 2010 Feb;50(2):110-22. doi: 10.1007/s00117-009-1893-0. Radiologe. 2010. PMID: 20157803 Review. German.
Cited by
-
Efficient TMS-Based Motor Cortex Mapping Using Gaussian Process Active Learning.IEEE Trans Neural Syst Rehabil Eng. 2021;29:1679-1689. doi: 10.1109/TNSRE.2021.3105644. Epub 2021 Aug 30. IEEE Trans Neural Syst Rehabil Eng. 2021. PMID: 34406942 Free PMC article.
-
Permanent deterioration of fine motor skills after the resection of tumors in the supplementary motor area.Neurosurg Rev. 2024 Mar 14;47(1):114. doi: 10.1007/s10143-024-02330-2. Neurosurg Rev. 2024. PMID: 38480549 Free PMC article.
-
Navigated Transcranial Magnetic Stimulation Motor Mapping Usefulness in the Surgical Management of Patients Affected by Brain Tumors in Eloquent Areas: A Systematic Review and Meta-Analysis.Front Neurol. 2021 Mar 4;12:644198. doi: 10.3389/fneur.2021.644198. eCollection 2021. Front Neurol. 2021. PMID: 33746895 Free PMC article.
-
Caffeine-Induced Global Reductions in Resting-State BOLD Connectivity Reflect Widespread Decreases in MEG Connectivity.Front Hum Neurosci. 2013 Mar 4;7:63. doi: 10.3389/fnhum.2013.00063. eCollection 2013. Front Hum Neurosci. 2013. PMID: 23459778 Free PMC article.
-
Language mapping with navigated repetitive TMS: proof of technique and validation.Neuroimage. 2013 Nov 15;82:260-72. doi: 10.1016/j.neuroimage.2013.05.018. Epub 2013 May 20. Neuroimage. 2013. PMID: 23702420 Free PMC article.
References
-
- Babiloni C, Carducci F, Cincotti F, Rossini PM, Neuper C, Pfurtscheller G, et al. Human movement-related potentials vs desynchronization of EEG alpha rhythm: a high-resolution EEG study. Neuroimage. 1999;10:658–665. - PubMed
-
- Beisteiner R, Windischberger C, Lanzenberger R, Edward V, Cunnington R, Erdler M, et al. Finger somatotopy in human motor cortex. Neuroimage. 2001;13:1016–1026. - PubMed
-
- Berger MS, Ojemann GA. Intraoperative brain mapping techniques in neuro-oncology. Stereotact Funct Neurosurg. 1992;58:153–161. - PubMed
-
- Berger MS, Ojemann GA, Lettich E. Neurophysiological monitoring during astrocytoma surgery. Neurosurg Clin N Am. 1990;1:65–80. - PubMed
-
- Carrabba G, Fava E, Giussani C, Acerbi F, Portaluri F, Songa V, et al. Cortical and subcortical motor mapping in rolandic and perirolandic glioma surgery: impact on postoperative morbidity and extent of resection. J Neurosurg Sci. 2007;51:45–51. - PubMed
