

Virological effectiveness and CD4+ T-cell increase over early and late courses in HIV infected patients on antiretroviral therapy: focus on HCV and anchor class received
- PMID: 22703595
- PMCID: PMC3409064
- DOI: 10.1186/1742-6405-9-18
Virological effectiveness and CD4+ T-cell increase over early and late courses in HIV infected patients on antiretroviral therapy: focus on HCV and anchor class received
Abstract
Background: The aim of this study was to explore the effects of HCV co-infection on virological effectiveness and on CD4+ T-cell recovery in patients with an early and sustained virological response after HAART.
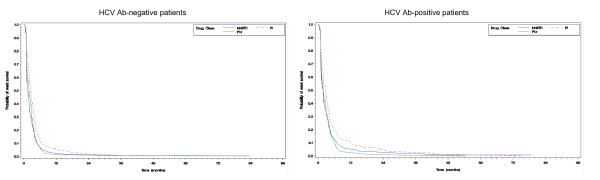
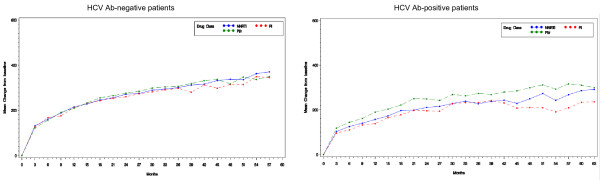
Methods: We performed a longitudinal analysis of 3,262 patients from the MASTER cohort, who started HAART from 2000 to 2008. Patients were stratified into 6 groups by HCV status and type of anchor class. The early virological outcome was the achievement of HIV RNA <500 copies/ml 4-8 months after HAART initiation. Time to virological response was also evaluated by Kaplan-Meier analysis. The main outcome measure of early immunological response was the achievement of CD4+ T-cell increase by ≥100/mm3 from baseline to month 4-8 in virological responder patients. Late immunological outcome was absolute variation of CD4+ T-cell count with respect to baseline up to month 24. Multivariable analysis (ANCOVA) investigated predictors for this outcome.
Results: The early virological response was higher in HCV Ab-negative than HCV Ab-positive patients prescribed PI/r (92.2% versus 88%; p = 0.01) or NNRTI (88.5% versus 84.7%; p = 0.06). HCV Ab-positive serostatus was a significant predictor of a delayed virological suppression independently from other variables, including types of anchor class. Reactivity for HCV antibodies was associated with a lower probability of obtaining ≥100/mm3 CD4+ increase within 8 months from HAART initiation in patients treated with PI/r (62.2% among HCV Ab-positive patients versus 70.9% among HCV Ab-negative patients; p = 0.003) and NNRTI (63.7% versus 74.7%; p < 0.001). Regarding late CD4+ increase, positive HCV Ab appeared to impair immune reconstitution in terms of absolute CD4+ T-cell count increase both in patients treated with PI/r (p = 0.013) and in those treated with NNRTI (p = 0.002). This was confirmed at a multivariable analysis up to 12 months of follow-up.
Conclusions: In this large cohort, HCV Ab reactivity was associated with an inferior virological outcome and an independent association between HCV Ab-positivity and smaller CD4+ increase was evident up to 12 months of follow-up. Although the difference in CD4+ T-cell count was modest, a stricter follow-up and optimization of HAART strategy appear to be important in HIV patients co-infected by HCV. Moreover, our data support anti-HCV treatment leading to HCV eradication as a means to facilitate the achievement of the viro-immunological goals of HAART.
Figures

References
-
- Bollepalli S, Mathieson K, Bay C, Hillier A, Post J, Van Thiel DH, Nadir A. Prevalence of risk factors for hepatitis C virus in HIV-infected and HIV/hepatitis C virus-coinfected patients. Sex Transm Infect. 2007;34:367–370. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
