

Evolution of coronary computed tomography radiation dose reduction at a tertiary referral center
- PMID: 22703931
- PMCID: PMC6849692
- DOI: 10.1016/j.amjmed.2011.10.036
Evolution of coronary computed tomography radiation dose reduction at a tertiary referral center
Abstract
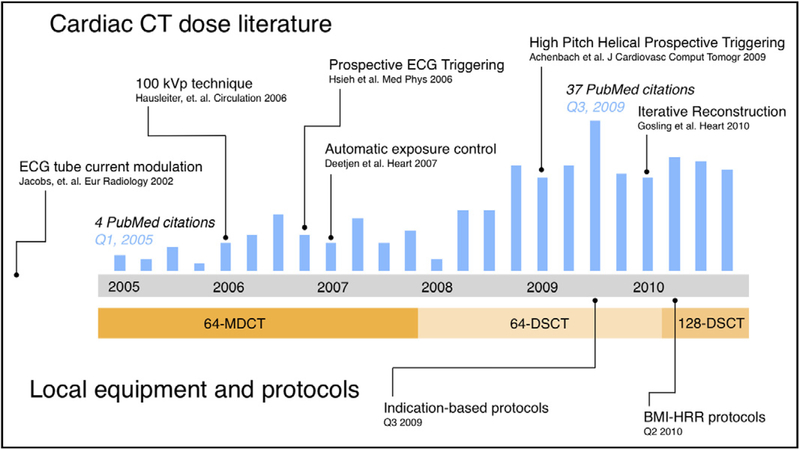
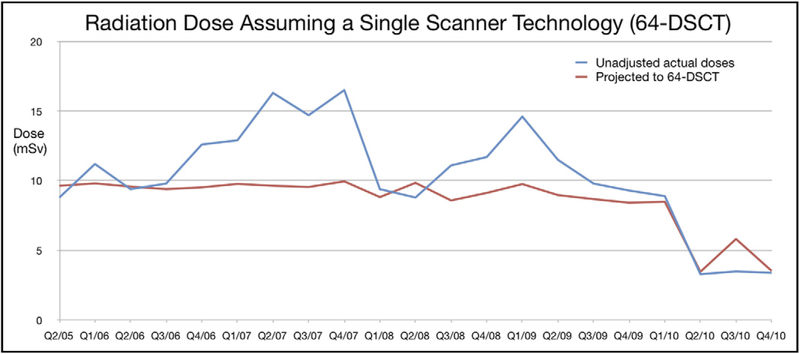
Purpose: We aimed to assess the temporal change in radiation doses from coronary computed tomography angiography (CCTA) during a 6-year period. High CCTA radiation doses have been reduced by multiple technologies that, if used appropriately, can decrease exposures significantly.
Methods: A total of 1277 examinations performed from 2005 to 2010 were included. Univariate and multivariable regression analysis of patient- and scan-related variables was performed with estimated radiation dose as the main outcome measure.
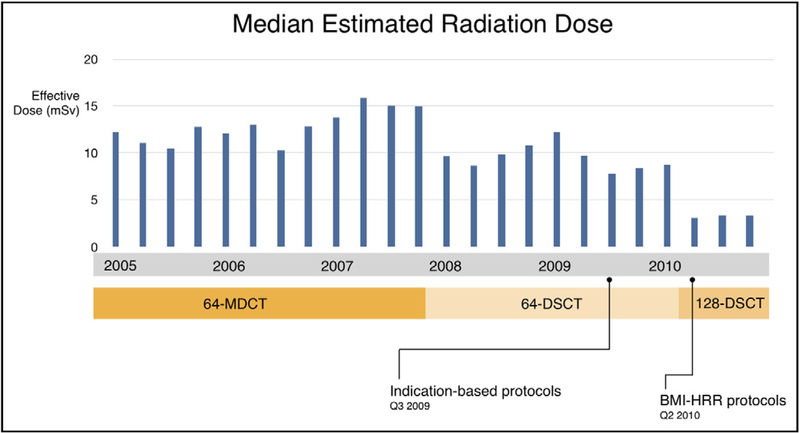
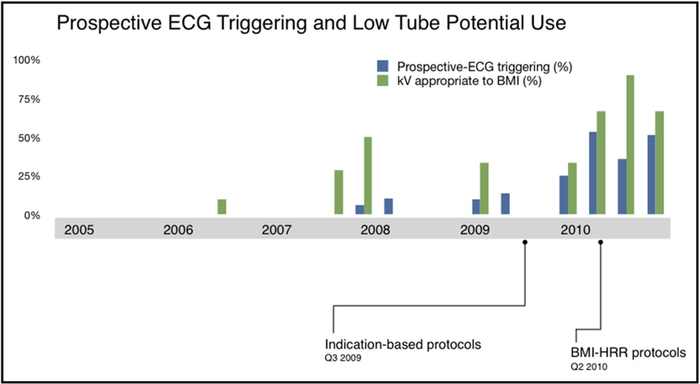
Results: Median doses decreased by 74.8% (P<.001), from 13.1 millisieverts (mSv) (interquartile range 9.3-14.7) in period 1 to 3.3 mSv (1.8-6.7) in period 4. Factors associated with greatest dose reductions (P<.001) were all most frequently applied in period 4: axial-sequential acquisition (univariate: -8.0 mSv [-9.7 to -7.9]), high-pitch helical acquisition (univariate: -8.8 mSv [-9.3 to -7.9]), reduced tube voltage (100 vs 120 kV) (univariate: -6.4 mSv [-7.4 to -5.4]), and use of automatic exposure control (univariate: -5.3 mSv [-6.2 to -4.4]).
Conclusions: CCTA radiation doses were reduced 74.8% through increasing use of dose-saving measures and evolving scanner technology.
Copyright © 2012 Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflict of Interest: None.
Figures
Comment in
-
Medical radiation safety: rational policy, irrational science.Am J Med. 2012 Aug;125(8):730-1. doi: 10.1016/j.amjmed.2012.01.010. Epub 2012 May 30. Am J Med. 2012. PMID: 22657562 No abstract available.
Similar articles
-
Radiation dose of coronary CT angiography with a third-generation dual-source CT in a "real-world" patient population.Eur Radiol. 2019 Aug;29(8):4341-4348. doi: 10.1007/s00330-018-5856-6. Epub 2018 Nov 30. Eur Radiol. 2019. PMID: 30506216
-
Submillisievert median radiation dose for coronary angiography with a second-generation 320-detector row CT scanner in 107 consecutive patients.Radiology. 2013 Apr;267(1):76-85. doi: 10.1148/radiol.13122621. Epub 2013 Jan 22. Radiology. 2013. PMID: 23340461 Free PMC article.
-
Radiation dose reduction by using 100-kV tube voltage in cardiac 64-slice computed tomography: a comparative study.Eur J Radiol. 2010 Jul;75(1):e51-6. doi: 10.1016/j.ejrad.2009.07.012. Epub 2009 Aug 9. Eur J Radiol. 2010. PMID: 19671491
-
Trends in radiation protection in CT: present and future status.J Cardiovasc Comput Tomogr. 2009 Nov-Dec;3 Suppl 2:S65-73. doi: 10.1016/j.jcct.2009.11.003. Epub 2009 Nov 15. J Cardiovasc Comput Tomogr. 2009. PMID: 20129519 Review.
-
Low-Dose Radiation Advances in Coronary Computed Tomography Angiography in the Diagnosis of Coronary Artery Disease.Curr Cardiol Rev. 2019;15(4):304-315. doi: 10.2174/1573403X15666190222163737. Curr Cardiol Rev. 2019. PMID: 30806322 Free PMC article. Review.
Cited by
-
Feasibility of a radiation dose conserving CT protocol for myocardial function assessment.Br J Radiol. 2014 Aug;87(1040):20130755. doi: 10.1259/bjr.20130755. Epub 2014 Jun 2. Br J Radiol. 2014. PMID: 24884727 Free PMC article.
-
Computed tomography-guided pericardiocentesis: a systematic review concerning contemporary evidence and future perspectives.Ther Adv Cardiovasc Dis. 2018 Nov;12(11):299-307. doi: 10.1177/1753944718792413. Epub 2018 Aug 15. Ther Adv Cardiovasc Dis. 2018. PMID: 30111248 Free PMC article.
-
Coronary CT Angiography as a Diagnostic and Prognostic Tool: Perspective from a Multicenter Randomized Controlled Trial: PROMISE.Curr Cardiol Rep. 2016 May;18(5):40. doi: 10.1007/s11886-016-0718-9. Curr Cardiol Rep. 2016. PMID: 26995403 Clinical Trial.
-
Sex differences in the effectiveness of early coronary computed tomographic angiography compared with standard emergency department evaluation for acute chest pain: the rule-out myocardial infarction with Computer-Assisted Tomography (ROMICAT)-II Trial.Circulation. 2013 Jun 25;127(25):2494-502. doi: 10.1161/CIRCULATIONAHA.113.001736. Epub 2013 May 17. Circulation. 2013. PMID: 23685743 Free PMC article. Clinical Trial.
-
Performance of a Deep Neural Network Algorithm Based on a Small Medical Image Dataset: Incremental Impact of 3D-to-2D Reformation Combined with Novel Data Augmentation, Photometric Conversion, or Transfer Learning.J Digit Imaging. 2020 Apr;33(2):431-438. doi: 10.1007/s10278-019-00267-3. J Digit Imaging. 2020. PMID: 31625028 Free PMC article.
References
-
- Brenner DJ, Hall EJ. Computed tomography—an increasing source of radiation exposure. N Engl J Med. 2007;357:2277–2284. - PubMed
-
- Min JK, Shaw LJ, Berman DS. The present state of coronary computed tomography angiography a process in evolution. J Am Coll Cardiol. 2010;55:957–965. - PubMed
-
- Tsai IC, Choi BW, Chan C, et al. ASCI 2010 appropriateness criteria for cardiac computed tomography: a report of the Asian Society of Cardiovascular Imaging Cardiac Computed Tomography and Cardiac Magnetic Resonance Imaging Guideline Working Group. Int J Cardiovasc Imaging. 2010;26(Suppl 1):1–15. - PubMed
-
- Carbonaro S, Villines TC, Hausleiter J, Devine PJ, Gerber TC, Taylor AJ. International, multidisciplinary update of the 2006 Appropriateness Criteria for cardiac computed tomography. J Cardiovasc Comput Tomogr. 2009;3:224–232. - PubMed
-
- Taylor AJ, Cerqueira M, Hodgson JM, et al. ACCF/SCCT/ACR/AHA/ASE/ASNC/NASCI/SCAI/SCMR 2010 appropriate use criteria for cardiac computed tomography. A report of the American College of Cardiology Foundation Appropriate Use Criteria Task Force, the Society of Cardiovascular Computed Tomography, the American College of Radiology, the American Heart Association, the American Society of Echocardiography, the American Society of Nuclear Cardiology, the North American Society for Cardiovascular Imaging, the Society for Cardiovascular Angiography and Interventions, and the Society for Cardiovascular Magnetic Resonance. J Am Coll Cardiol. 2010;56: 1864–1894. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
