

Optimized fluid management improves outcomes of pediatric burn patients
- PMID: 22703982
- PMCID: PMC3465500
- DOI: 10.1016/j.jss.2012.05.058
Optimized fluid management improves outcomes of pediatric burn patients
Abstract
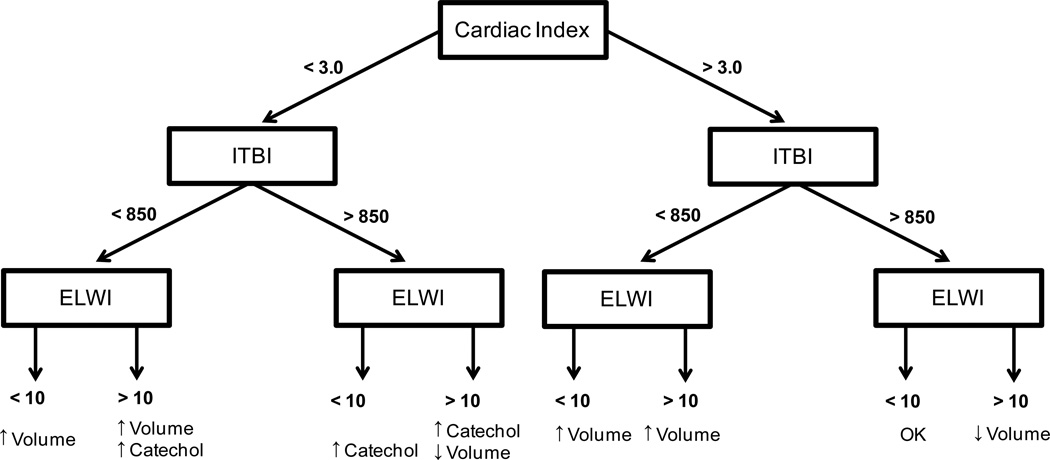
Background: One of the major determinants for survival of severely burned patients is appropriate fluid resuscitation. At present, fluid resuscitation is calculated based on body weight or body surface area, burn size, and urinary output. However, recent evidence suggests that fluid calculation is inadequate and that over- and under-resuscitations are associated with increased morbidity and mortality. We hypothesize that optimizing fluid administration during the critical initial phase using a transcardiopulmonary thermodilution monitoring device (pulse contour cardiac output [PiCCO]; Pulsion Medical Systems, Munich, Germany) would have beneficial effects on the outcome of burned patients.
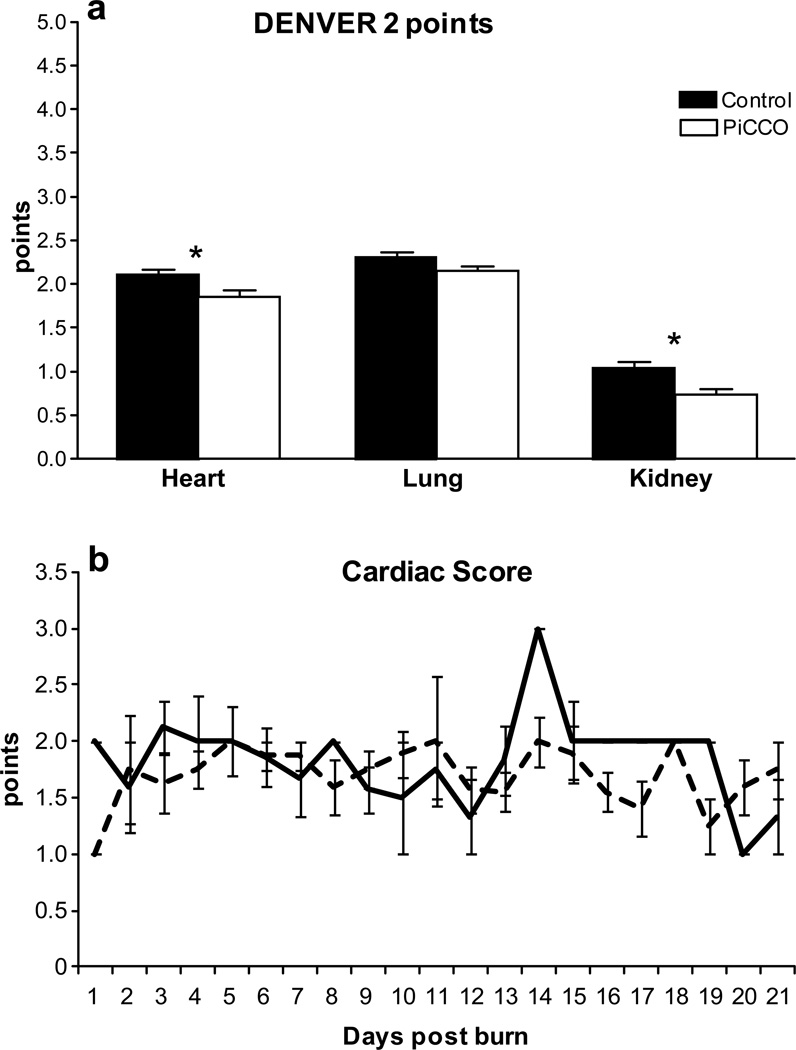
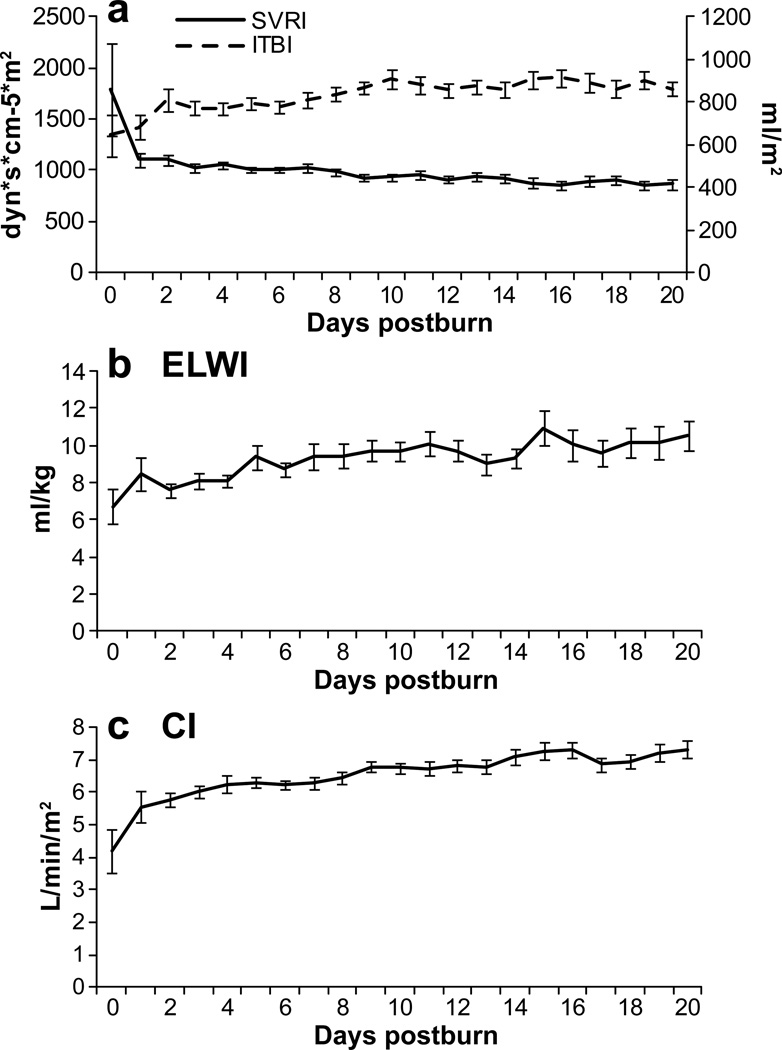
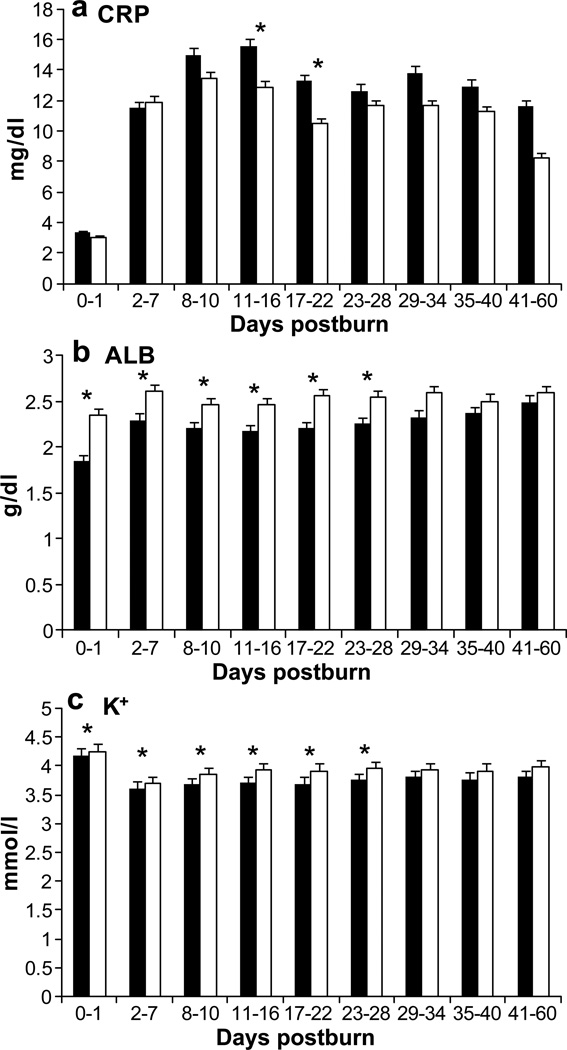
Methods: A cohort of 76 severely burned pediatric patients with burns over 30% of the total body surface area who received adjusted fluid resuscitation using the PiCCO system were compared with 76 conventionally monitored patients (C). Clinical hemodynamic measurements, organ function (DENVER2 score), and biomarkers were recorded prospectively for the first 20d after burn injury.
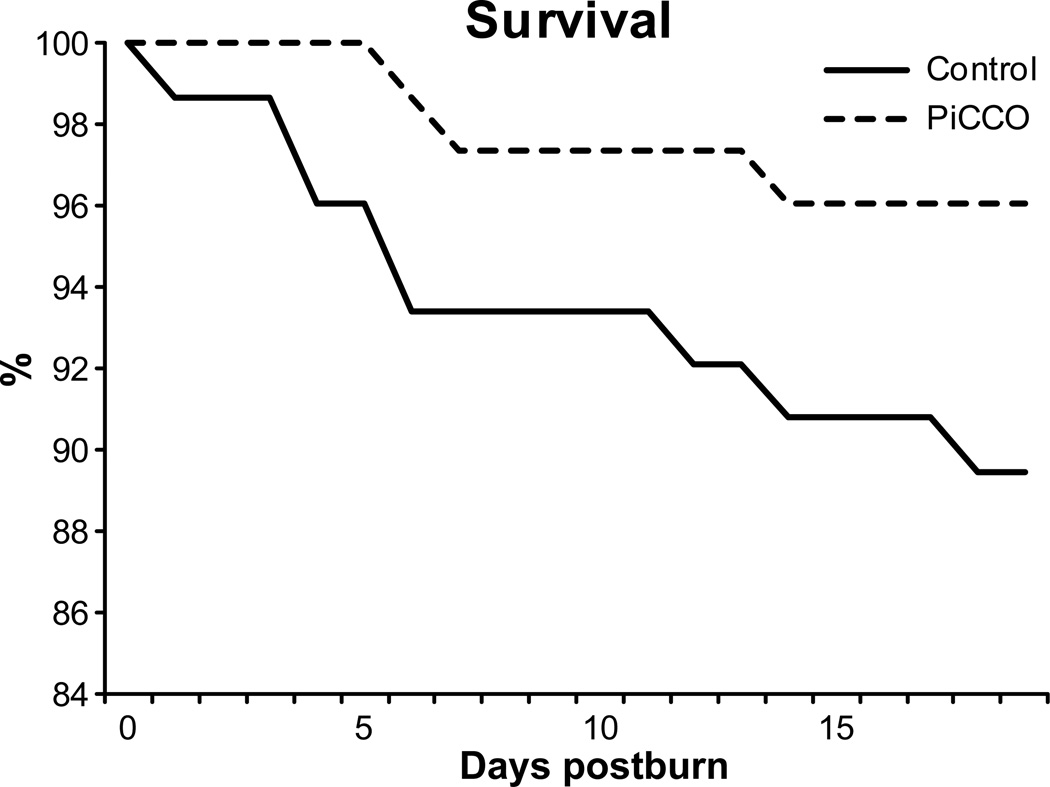
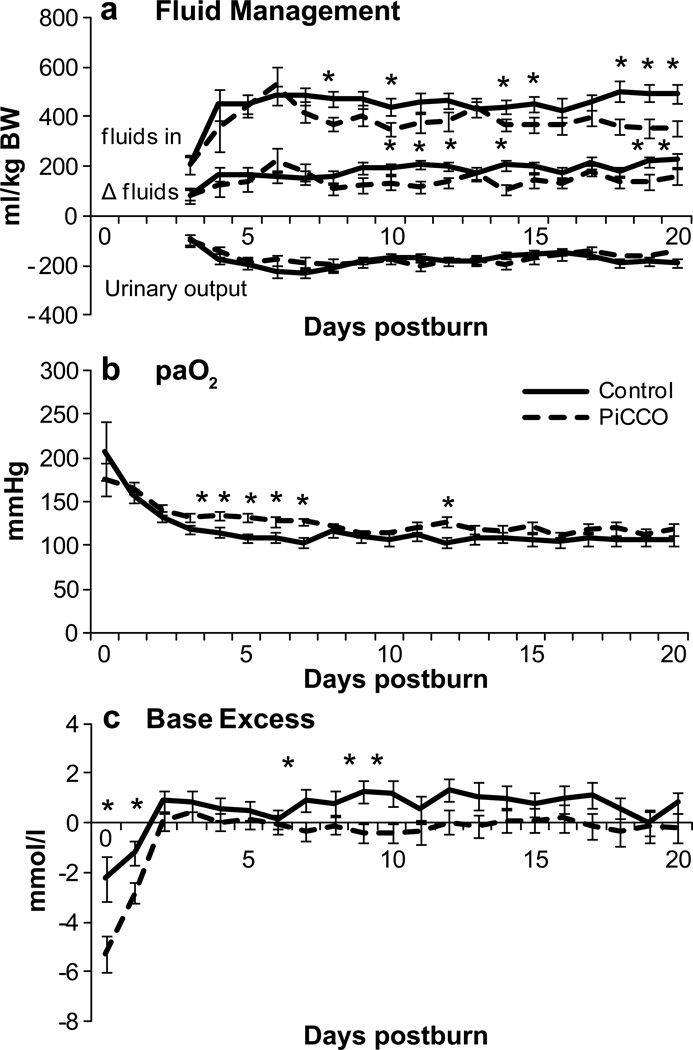
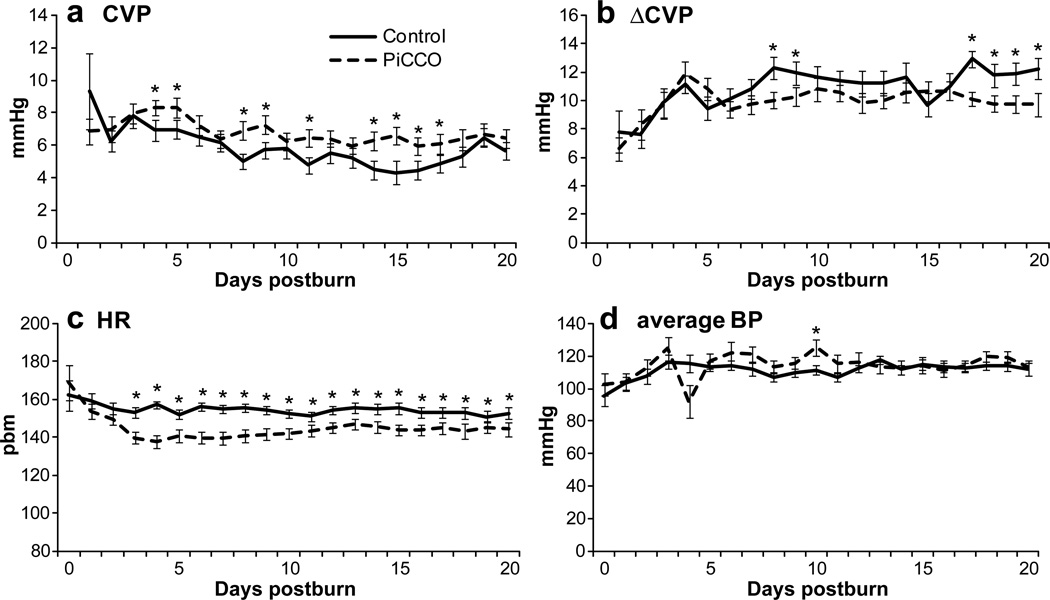
Results: Both cohorts were similar in demographic and injury characteristics. Patients in the PiCCO group received significantly less fluids (P<0.05) with similar urinary output, resulting in a significantly lower positive fluid balance (P<0.05). The central venous pressure in the PiCCO group was maintained in a more controlled range (P<0.05), associated with a significantly lower heart rate and significantly lower incidence of cardiac and renal failure (P<0.05).
Conclusions: Fluid resuscitation guided by transcardiopulmonary thermodilution during hospitalization represents an effective adjunct and is associated with beneficial effects on postburn morbidity.
Copyright © 2013 Elsevier Inc. All rights reserved.
Figures
Similar articles
-
[Effect of fluid resuscitation guided by pulse contour cardiac output monitoring technology on organ function in extremely severe burn patients].Zhonghua Shao Shang Za Zhi. 2020 Oct 20;36(10):939-946. doi: 10.3760/cma.j.cn501120-20190811-00345. Zhonghua Shao Shang Za Zhi. 2020. PMID: 33105946 Clinical Trial. Chinese.
-
[Application of pulse contour cardiac output monitoring technology in fluid resuscitation of severe burn patients in shock period].Zhonghua Shao Shang Za Zhi. 2021 Feb 20;37(2):136-142. doi: 10.3760/cma.j.cn501120-20200908-00403. Zhonghua Shao Shang Za Zhi. 2021. PMID: 33498100 Chinese.
-
[Clinical significance of pulse contour cardiac output monitoring technology in guiding fluid replacement during shock stage of extensive burn].Zhonghua Shao Shang Za Zhi. 2019 Jun 20;35(6):434-440. doi: 10.3760/cma.j.issn.1009-2587.2019.06.007. Zhonghua Shao Shang Za Zhi. 2019. PMID: 31280536 Clinical Trial. Chinese.
-
Burn shock resuscitation.World J Surg. 1992 Jan-Feb;16(1):16-23. doi: 10.1007/BF02067109. World J Surg. 1992. PMID: 1290260 Review.
-
Hemodynamic monitoring by transpulmonary thermodilution and pulse contour analysis in critically ill children.Pediatr Crit Care Med. 2011 Jul;12(4):459-66. doi: 10.1097/PCC.0b013e3182070959. Pediatr Crit Care Med. 2011. PMID: 21263372 Review.
Cited by
-
Glucose Control in Severely Burned Patients Using Metformin: An Interim Safety and Efficacy Analysis of a Phase II Randomized Controlled Trial.Ann Surg. 2016 Sep;264(3):518-27. doi: 10.1097/SLA.0000000000001845. Ann Surg. 2016. PMID: 27355267 Free PMC article. Clinical Trial.
-
Correlation between invasive and noninvasive blood pressure measurements in severely burned children.Burns. 2018 Nov;44(7):1787-1791. doi: 10.1016/j.burns.2018.03.001. Epub 2018 Aug 25. Burns. 2018. PMID: 30153960 Free PMC article.
-
Prediction of outcome in patients with ARDS: A prospective cohort study comparing ARDS-definitions and other ARDS-associated parameters, ratios and scores at intubation and over time.PLoS One. 2020 May 6;15(5):e0232720. doi: 10.1371/journal.pone.0232720. eCollection 2020. PLoS One. 2020. PMID: 32374755 Free PMC article.
-
The P50 Research Center in Perioperative Sciences: How the investment by the National Institute of General Medical Sciences in team science has reduced postburn mortality.J Trauma Acute Care Surg. 2017 Sep;83(3):532-542. doi: 10.1097/TA.0000000000001644. J Trauma Acute Care Surg. 2017. PMID: 28697015 Free PMC article.
-
Transpulmonary Thermodilution Versus Transthoracic Echocardiography for Cardiac Output Measurements in Severely Burned Children.Shock. 2016 Sep;46(3):249-53. doi: 10.1097/SHK.0000000000000627. Shock. 2016. PMID: 27058051 Free PMC article.
References
-
- Hoskins SL, Elgjo GI, Lu J, et al. Closed-loop resuscitation of burn shock. J Burn Care Res. 2006;27:377. - PubMed
-
- Gore DC, Hawkins HK, Chinkes DL, et al. Assessment of adverse events in the demise of pediatric burn patients. J Trauma. 2007;63:814. - PubMed
-
- Brusselaers N, Monstrey S, Colpaert K, et al. Outcome of acute kidney injury in severe burns: a systematic review and meta-analysis. Intensive Care Med. 2010;36:915. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
